In this month’s Endodontics 101 column, Josette Camilleri discusses the properties and uses of hydraulic cements in endodontics.
Introduction
Endodontic procedures are divided into pulp therapy, non-surgical root canal treatment and surgical treatment.
The materials that are most indicated for the following procedures are hydraulic cements. They are:
- Vital pulp therapy
- Regenerative endodontics
- Root canal obturation using the gutta-percha point and root canal sealer
- The management of immature apices, either by apical plugs
- Apical surgery
- Perforation repair.
This article overviews the properties and uses of hydraulic cements in endodontics.
Main features
The main features of hydraulic cements are the need of water to set and also environmental moisture to allow the materials to develop their properties.
This has clinical implications because, when performing endodontic procedures, the environment changes with the use other materials and irrigating solutions. There is also the presence of blood and tissue fluids that effect the material properties.
A classification for these materials has been proposed based on the material chemistry. As a result, this helps clinicians to understand the differences in the types of material as this has clinical implications.
Furthermore, the classification also subdivides the materials according to use which is coronal, intra-radicular and extra-radicular.
Material composition and presentation
Most of the hydraulic cements are composed of a powder and liquid.
The power comprises a cement and radiopacifier and may contain additives depending on the material clinical use.
The liquid is water which may also contain additives to enhance the material properties.

Some materials use non-aqueous vehicles, and these can be delivered in syringes facilitating delivery.
There are three types of presentations, namely powder and liquid (Figure 1a), automix syringes (Figure 1b) and single syringe/container systems which can be of different consistencies (Figure 1c).

The automix syringes use resins as vehicles and, as such, cannot be classified as hydraulic cements as the primary reaction is the resin reaction.

Hydraulic cements can have different chemistries. The tricalcium and dicalcium silicate chemistry is the one that is most investigated in dentistry.
The materials used for endodontic procedures have a tricalcium silicate chemistry. This means, when mixed with water as in the powder/liquid or absorbs moisture from the environment in the single syringe system, it will hydrate and form calcium silicate hydrate and calcium hydroxide.
The clinicians need to be careful to ensure that the materials they choose for the procedures have the tricalcium silicate chemistry.
Materials containing bismuth oxide should not be used for any endodontic procedure. This is due to the reactivity of bismuth oxide with endodontic irrigation solutions particularly sodium hypochlorite and also in contact with collagen in the tooth structure.
Clinical use
Intra-coronal use
The application of hydraulic calcium silicate cements intra-coronally includes their use for vital pulp therapy and regenerative endodontic procedures.
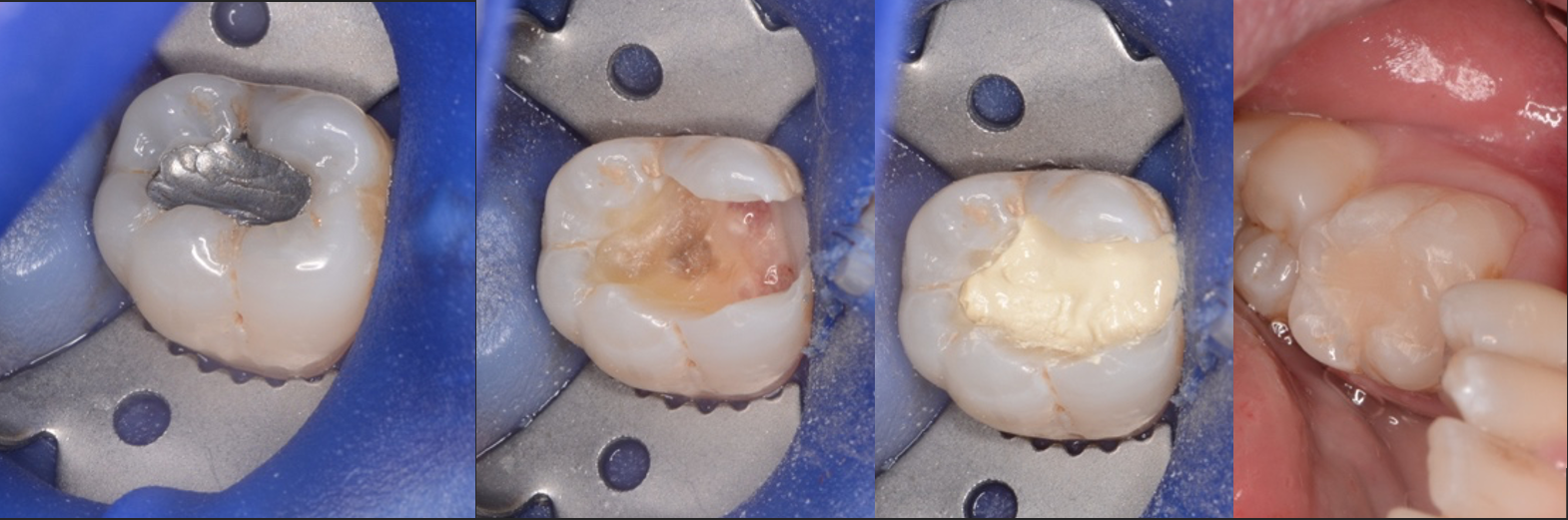
The use of hydraulic cement for vital pulp therapy requires a specific clinical protocol.
This includes the following steps:
- Proper diagnosis which may be limited due to the simplicity of the tests and lack of correlation between the symptoms and signs and pulp status
- Removal of all caries following the American Association of Endodontists guidelines as all evidence shows that the full removal of caries leads to better outcomes as summarised in a recent review article
- Dentine cleansing with sodium hypochlorite and ethylene diamine tetracetic acid
- Management of the dental pulp if necessary. Use of sodium hypochlorite reduces bacterial load
- Placement of a fast setting, bismuth oxide free hydraulic calcium silicate cement. If Biodentine is used, five drops of liquid need to be placed with the powder in the capsule and mixed in Septodont mixer for 30s
- Selective etching with a five second etch of the hydraulic calcium silicate pulp preservation material and a total etch of the dentine and enamel. The enamel etch can be undertaken prior to the placement of the hydraulic cement to avoid the washing out of the material
- Application of a dentine bonding agent or use of a resin modified glass ionomer over hydraulic cement and placement of a composite resin restoration.
If the restoration cannot be undertaken on the first visit, the tooth can be restored fully with Biodentine.
It is not recommended to use a zinc oxide eugenol or a glass ionomer temporary restorative material over the Biodentine. This is because this interferes with the material setting.
For regenerative endodontic procedures, the clinical guidance by the European Society of Endodontology is recommended. The hydraulic cements are used as barriers and the same principles as those outlined for vital pulp therapy are recommended.
Intra-radicular use
The intra-radicular use of the hydraulic cements is for root canal obturation where they are recommended to be used in single cone obturation technique. In addition, they are recommended as an apical plug for management of immature apices.
The material features for such procedures are adequate flow, radiopacity and antimicrobial characteristics. The presentation of root canal sealers varies from powder-liquid to single syringe devices.
Heat carriers used for warm vertical compaction techniques cause desiccation of hydraulic sealers that are in powder to liquid format with the single syringe ones being more resistant to heat.
The clinical procedure and tooth preparation are similar for both procedures.
The following steps are recommended:
- Root canal debridement with copious irrigation with sodium hypochlorite
- Use of ethylene diamine tetracetic acid to remove smear layer. This is specifically important when using single syringe sealers as the removal of smear layer allows the dentine fluid to re-enter into the root canal enabling the sealer to hydrate. Unless the sealer hydrates, the antimicorbial properties are compromised
- Final irrigation with sterile water. This is done to avoid leaving chemicals that may interfere with the hydration in situ’. Since the hydraulic cements are susceptible to environmental changes, the obturation and choice of sealers needs to be matched with the irrigation protocol
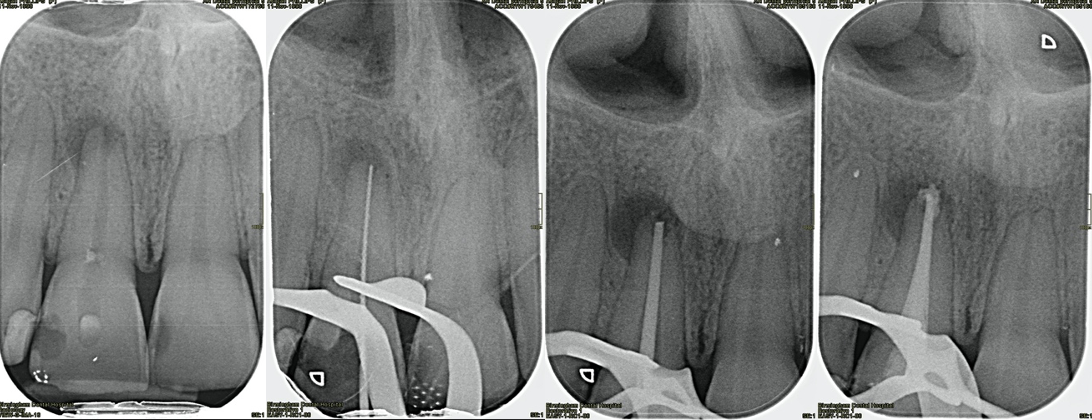
- For single cone obturation a cone fit radiograph is taken to check how the cone adapts to the space in the root canal. The sealer is placed at mid-root level. Since the hydraulic cements are water-based there is a tendency for overfill which should be avoided. A typical single cone obturation clinical case is shown in Figure 3
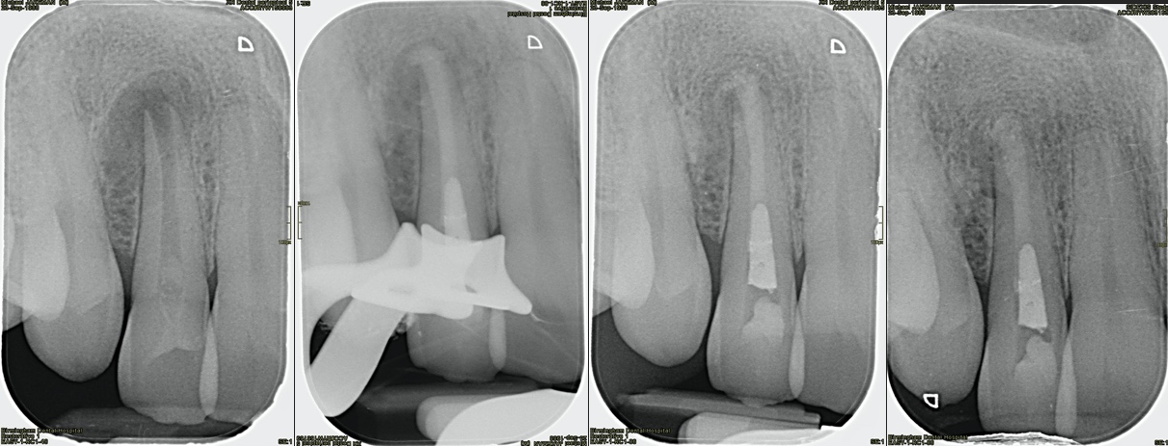
- For apical plugs in management of immature permanent teeth, the hydraulic cement is packed with a long shank plugger without pressure. Biodentine has adequate handling properties so it can be placed at the canal orifice and then pushed downwards with the pre-measured long shank pluggers. MTA is more difficult to place and necessitates the use of a carrier to place the material. A plug of approximately 4-5 mm should be placed. The rest of the root canal can be obturated with syringable thermoplasticized gutta-percha. A clinical case is shown in Figure 4.
Extra-radicular use
Hydraulic cements were developed for blocking the communication between the root canal and the periodontal ligament space in reparative procedure. For example, root-end surgery and perforation repair.
But despite this, there is no research on an optimised clinical protocol.
A collection of a few failed cases indicates that the hydraulic cements used for such procedures tend to be very sensitive to the environment. In addition, they may not set or be washed out with time leading to case failure.
Conclusions
Hydraulic cements are unique materials used in endodontic practice.
They are susceptible to the environmental moisture. Therefore, an appropriate clinical protocol is necessary to optimise the material properties and avoid case failure.
Not all hydraulic cements have the same chemistry, therefore the interactions may differ.
Contact [email protected] for references.
Catch up with the Endodontics 101 series:
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

