Douglas Benn explores Stafne bone cavities and how they show up in a CBCT scan.
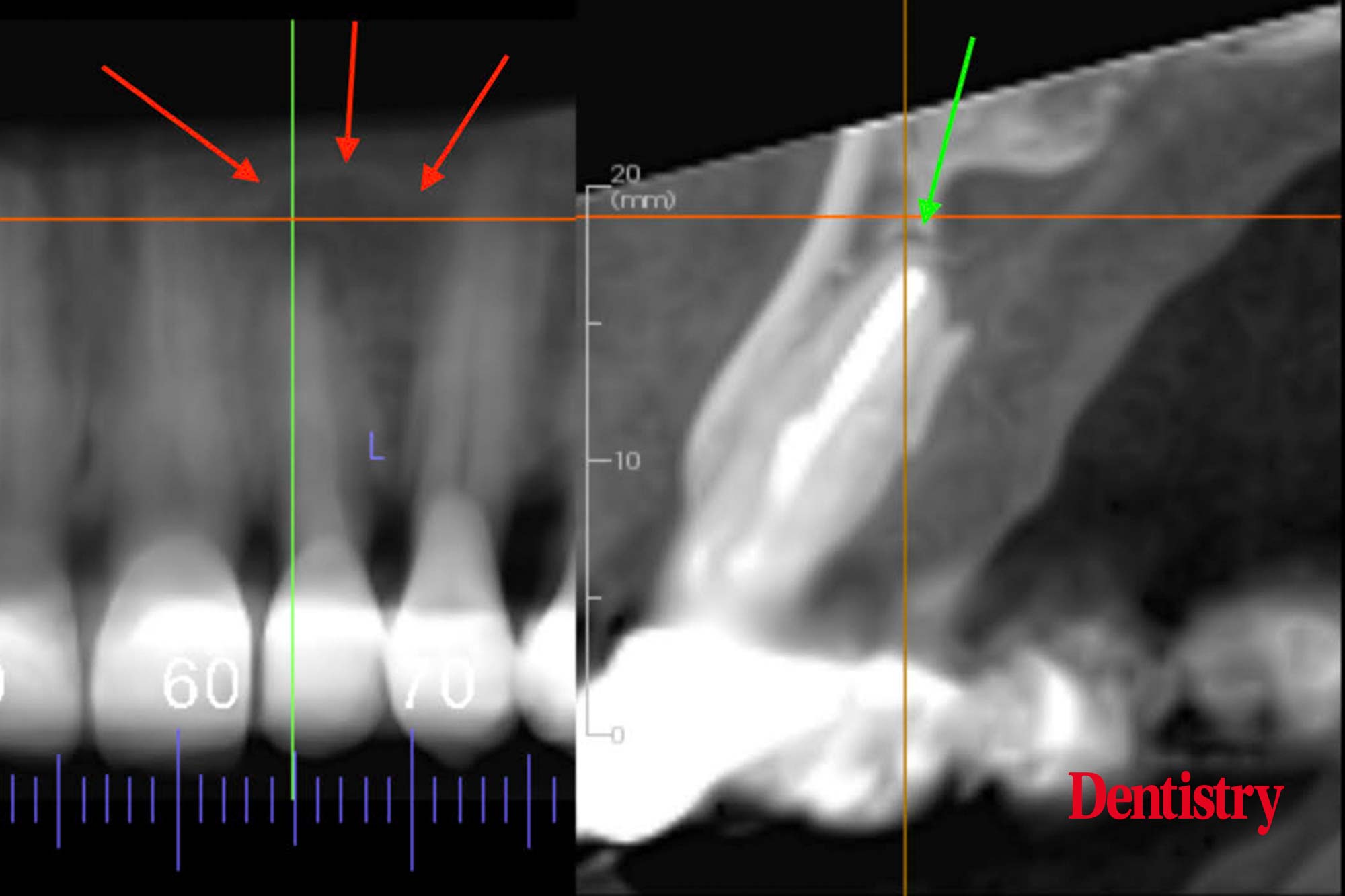 Two images, pre-extraction of the UL2.
Two images, pre-extraction of the UL2.
The left is a reconstructed cropped panoramic CBCT providing an image similar to a periapical intraoral radiograph.
The red arrows show the outline of a well defined corticated unilocular apical radiolucency of UL2 (three red arrows).
However, the right image is a cropped reconstructed sectional alveolar arch. It shows the UL2 apex has a 0.5 to 1.0mm radiolucency (green arrow).
The image also shows that the lamina dura is intact and not part of the large palatal concavity superior to the apex.
The radiolucency is very small and probably from fibrous healing of apex. But may also be granulation tissue from chronic apical periodontitis.
At this stage with no symptoms, the correct management is to monitor this six months later with a periapical radiograph to see if there is any radiographic change.
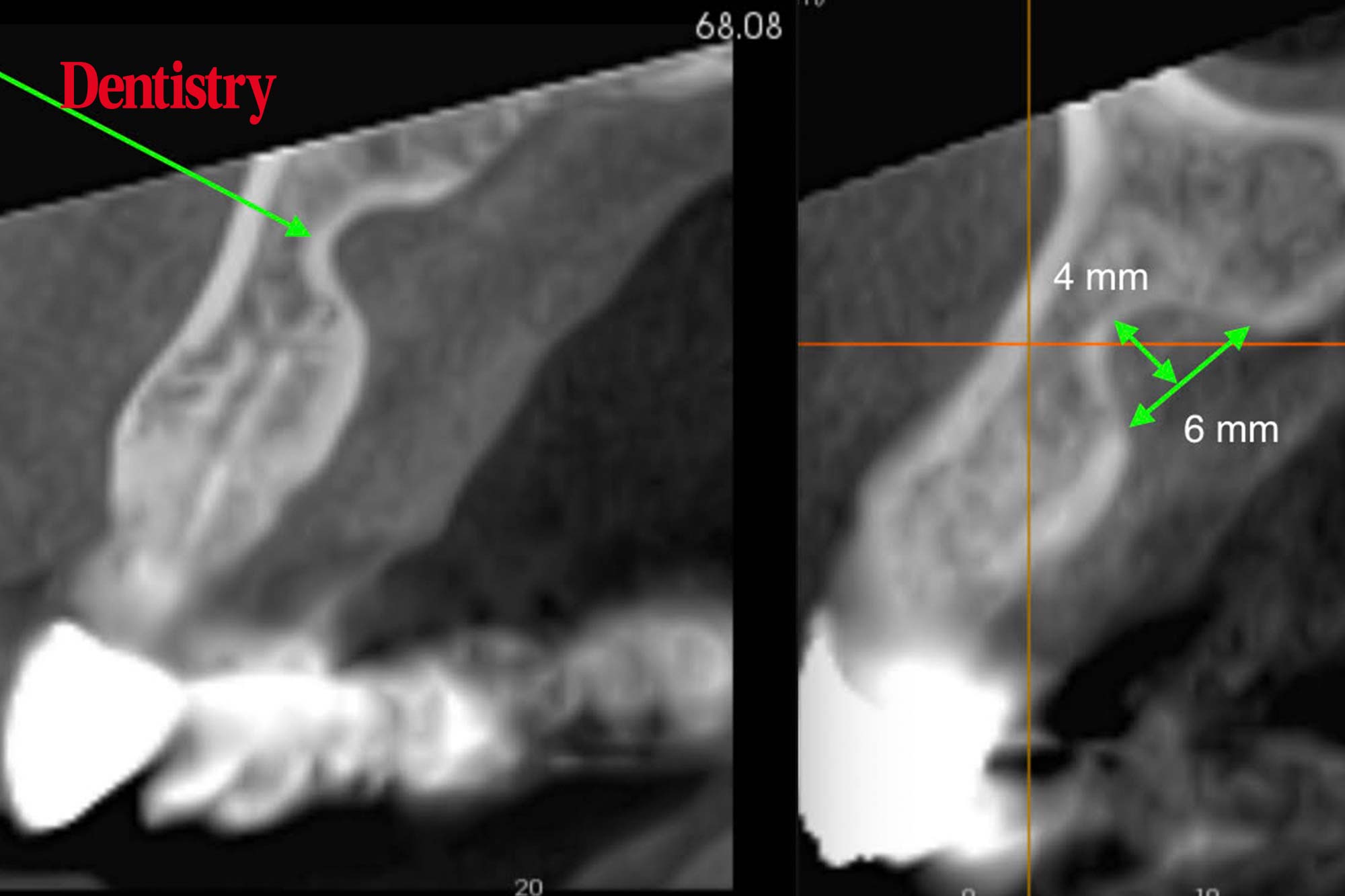
Two reconstructed CBCT cross sectional alveolar arch images made six months apart.
The left is pre-extraction UL2 and the right six months later, post extraction UL2.
Notice that both images have a well defined corticated concavity; in the palatal side of the alveolar bone ridge approximately 4mm wide by 6mm deep.
A detailed examination of cross sectional slices across the concavity confirmed that the bone concavity has not changed over a six-month time interval.
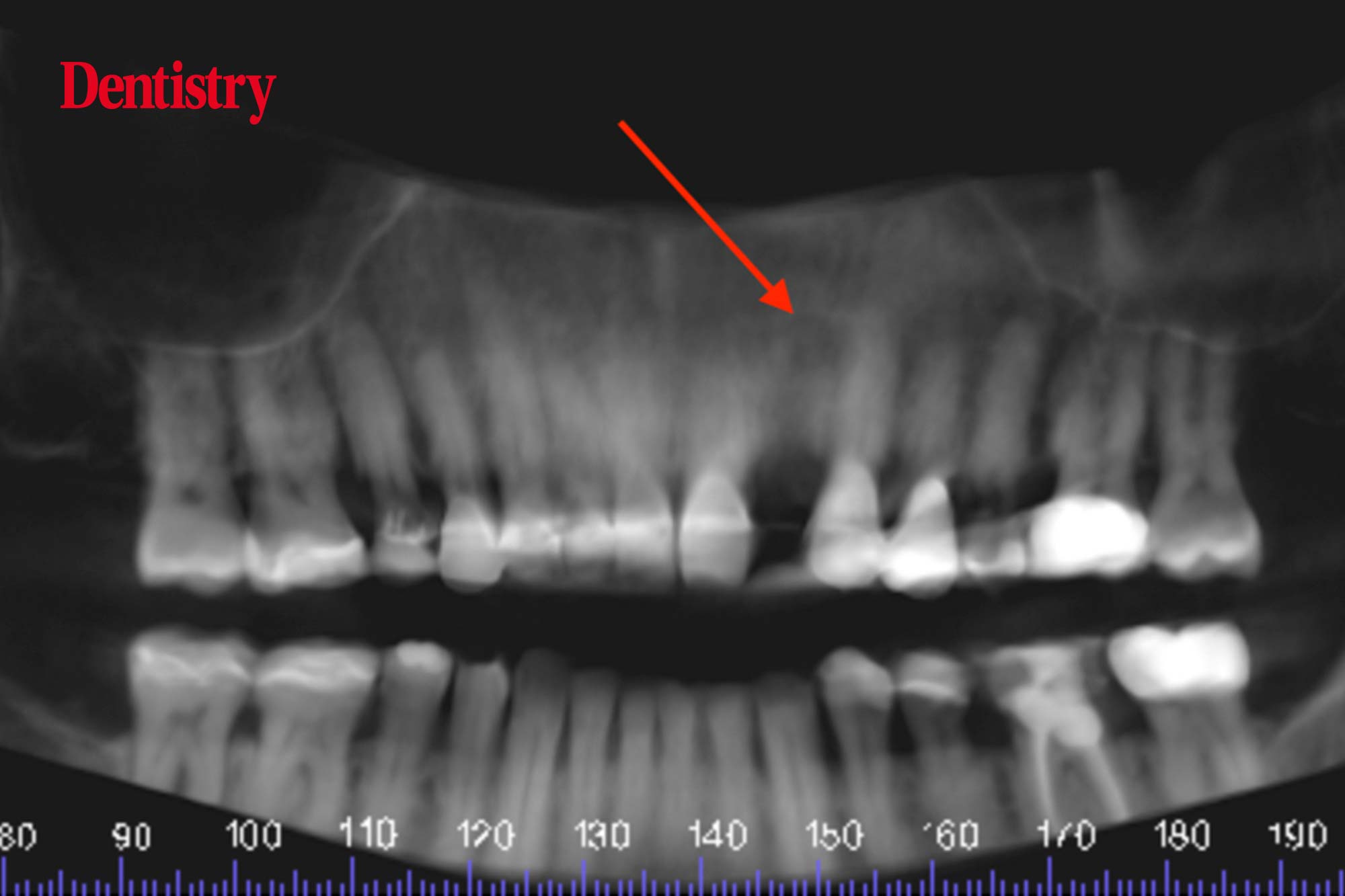
Post extraction CBCT reconstructed panoramic image showing circular radiolucency at edentulous UL2 apical region (red arrow).
Diagnosis
- The large well defined corticated bone concavity palatal to the apex of UL2 is a Stafne bone cavity. These are benign developmental defects. They occur more frequently in men, 6:1 male:female. And usually in the posterior mandible on the lingual surface and inferior to the mandibular canal. They usually contain fat, salivary gland or vascular tissues. However, I have seen them in the anterior mandible across the midline lingual region and now in the palate. As long as they remain well corticated and do not increase in size, they do not require treatment. Another CBCT just off the anterior maxilla region should be made six to 12 months after the first discovery or sooner if there are signs or symptoms. Providing the clinician observes no change, then this requires no further monitoring
- The small periapical radiolucency of UL2 required no treatment. It was a chance asymptomatic finding. A good periapical radiograph would show that the apical lamina dura was still intact and it would probably show no widening of the PLS. This would indicate that the larger well corticated Stafne bone defect was unlikely to be associated with apical pathology, which the CBCT would confirm.
For more information visit dental-scan.co.uk.

