
Philippe Sleiman explores the uses of nickel titanium files for a simplified approach to complex root canal treatment.
Since nickel titanium (NiTi) files were introduced into root canal therapy, engineers have been seeking the perfect design and combination for optimal root canal therapy. Heat treatment and twisting of NiTi was a major breakthrough in this field. It opened up the era of heat treatment for rotary files. Now almost all files in the market are heat-treated. This creates great flexibility but puts aside cutting efficiency, cutting being the major task for rotary files in shaping canals.
The Traverse and now ZenFlex file systems (both Kerr) are produced using a novel heat treatment that combines cutting efficiency and flexibility in one file and in the necessary places. This new technology in heat treatment adds value to our daily work. Ultimately what matters is the treatment that we offer to our patients. Safety and cutting efficiency are apparent when using these files. This allows me to use a rather simplified approach for treating the complex root canal anatomy. In this article, I will demonstrate this approach with reference to several cases.
Orifice opening
The orifice opening is done with the 25/.08 Traverse file, which has a maximum flute diameter of 1mm. This is a file that I use in almost all of my cases. In straight canals, it goes as deep as it can. In curved canals, it is limited to working above the curve.
For straight canals, ZenFlex offers a wide range of sizes, from 20 to 55, in both .04 taper and .06 taper. After using the ZenFlex for some time, the dentist can evaluate the size that he or she likes to use according to his or her experience and preferences and can use one ZenFlex file to finish the shaping.
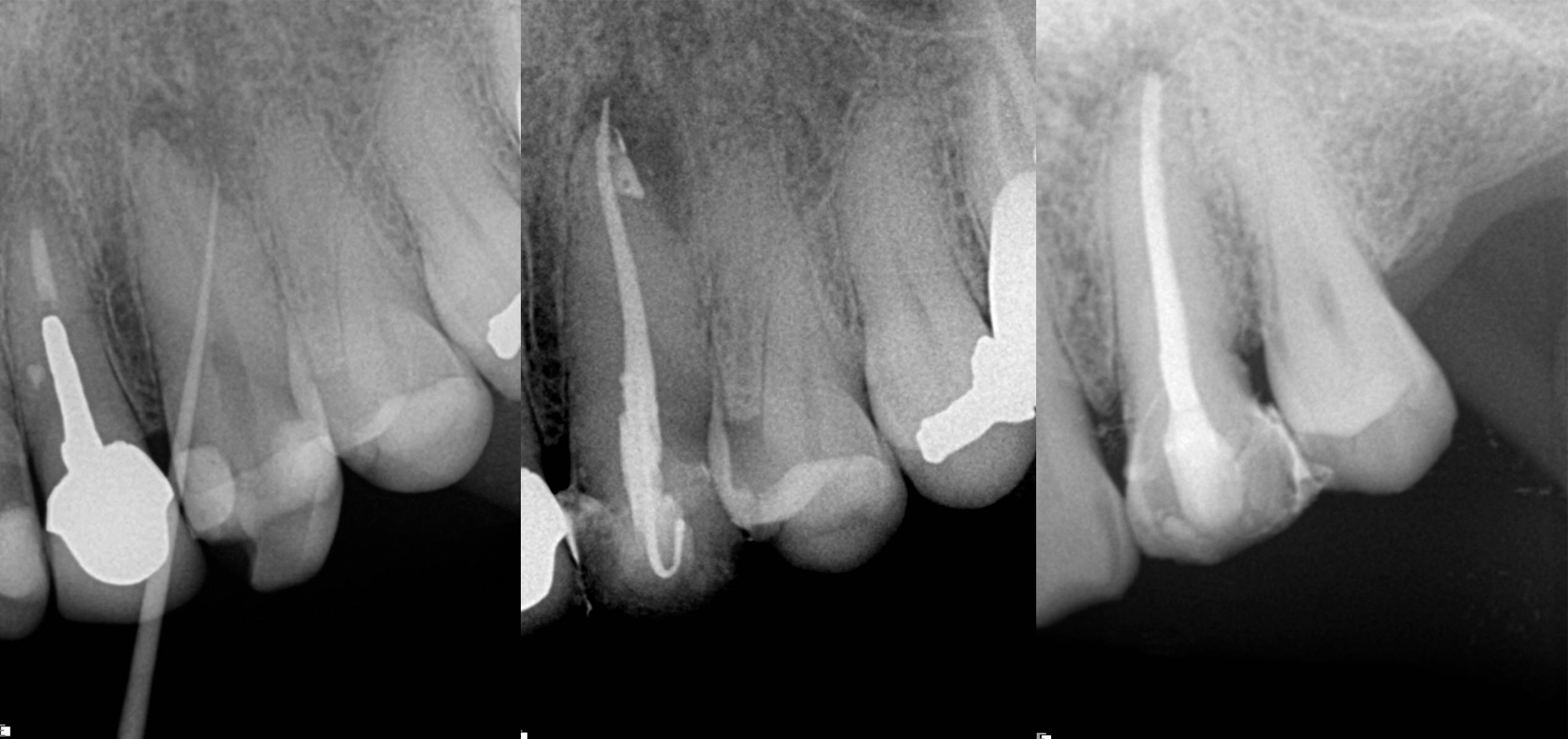
In this first example, the patient was referred for treatment of a sinus tract of the anterior maxilla (Fig. 1). A gutta-percha cone was placed inside the fistula, showing the way to the infection site. This was a straightforward case, prepared using the 25/.08 Traverse file in the upper part of the root canal, followed by a 10 K-File (Kerr) to determine the working length and then a 40/.06 Traverse file taken to working length. Naturally, treatment involved complete chemical preparation and 3D sealing of the root canal space (Fig. 2).
Single-file technique
The next example was also a straightforward case. This was a maxillary lateral incisor with a necrotic pulp and a slightly resorbed apex. A 55/.06 ZenFlex file was used in a single-file technique to treat this canal (Fig. 3).
In molars and narrow canals, a simple sequence is required in order to perform shaping. It can start with the 25/.08 Traverse file, taken to justabove the curve, especially in mesial canals. Using a K-File, the dentist can determine the working length using an apex locator and use this length for preparation with rotary files. The K-File is also used to achieve patency. The second rotary file is the 13/.06 Traverse file, taken to working length,followed by the 20/.06 and 25/.06 ZenFlex files, also taken to working length. If the dentist is following an apical enlargement regime, a 30/.04 ZenFlex file can be used for the apical area.

Maxillary second molars
Maxillary second molars are in my opinion one of the most challenging teeth to treat because of their position and unpredictable anatomy. In this example case, the patient was referred for irreversible pulpitis (Fig. 4). Looking at the preoperative radiograph, we can see the curvature of especially the mesial and palatal root canals. The sequence used was as described before, starting with the 25/.08 Traverse orifice opener as deep as it goes and just above the curve, followed by a 8 K-File for working length determination and the 13/.06 Traverse file used to working length in all canals.

During the use of the 13/.06 Traverse file, I did not feel much resistance, so I decided to go ahead with the .06 taper sequence. The next file was the 20/.06 ZenFlex, followed by the 25/.06 ZenFlex file. Personally, I believe in apical enlargemen. For that reason, I used the 30/.04 ZenFlex file as the final enlargement file in this case. I used a medium cone as the master cone and achieved 3D sealing of the system (Fig. 5). Of course, I performed complete chemical preparation, according to my sequence, during the procedure.
Narrow canals
In very narrow canals, the .06 taper ZenFlex file will be replaced by the .04 taper one. This reduces taper lock, which occurs when a large file is trapped inside a single or a double canal curve. This can create a great deal of torsional stress and bending stress on the same spot, leading to severe damage of the file and even to file separation. The sequence is use of the 25/.08 Traverse file in the straight part of the canal, followed by 8 and 10 K-Files, taken to working length. The 13/.06 Traverse file opens the way for the 20/.04ZenFlex file, which is followed by the 25/.04 ZenFlex file and additionally the 30/.04 ZenFlex file for apical enlargement. A medium or fine-medium cone can be adapted as the master cone.

Accessing narrow canals
In this example case, the patient was referred by his treating dentist, who had penetrated deep into the roots in trying to find the canals and was not successful, but fortunately no perforation had occurred (Fig. 6). Under the microscope and using ultrasonic tips, the canals were made accessible. On the radiograph, we can see that the canals, especially the mesial ones, are narrow and have small curves, particularly apically. The real challenge in this case was maintaining the original shape of the canal.
For those reasons, the sequence with the .04 taper was chosen. Treatment was initiated with the 25/.08 Traverse orifice opener, followed by a 8 K-File for working length determination. The 13/.06 Traverse file was used all the way to the end of the working length, followed by the 20/.04 and 25/.04 ZenFlex files, both taken to working length. For apical enlargement, the 30/.04 ZenFlex file was used.

A medium cone was used as the master cone in the distal root, and fine-medium cones were used in the mesial root. A full sequence of irrigation was used during the treatment, and the system, which included a deep isthmus between the mesial roots, was filled in multiple levels from the middle to the apex, achieving beautiful 3D obturation (Fig. 7).
For more information about the files used, visit www.kerrdental.com/en-uk.

