Satnam Singh Virdee shares his guide to making confident, informed decisions about endodontic retreatment.
General, specialist and consultant practitioners of varying dental disciplines frequently examine root filled teeth that potentially require endodontic retreatment. Treatment planning for these cases can nevertheless prove challenging due to patients presenting with a broad range of symptoms, clinical signs and radiographic features.
The following communication thus aims to assist practitioners with such decision-making processes with particular emphasis on determining when to and when not to proceed with endodontic retreatment.
Indications for retreatment
As per the European Society of Endodontology (ESE) 2006 quality guidelines, there are two indications for endodontic retreatment:
1. ‘Inadequate root canal filling with clinical and/or radiological findings of developing/persisting apical periodontitis’
The rationale for this pathological indication is to reduce the intraradicular microbial load to a threshold that is compatible with healing in a root filled tooth with active periradicular disease.
In order to fulfil this definition and proceed with orthograde retreatment, clinical and radiographic findings should reveal:
- A tooth that exhibits symptoms typical of active endodontic pathology (ie pain, tenderness to percussion or palpation, sinus or diffuse swelling)
- Pathology that is likely originating from an intraradicular source (ie no recollection of rubber dam use, poor quality coronal seal or primary root filling)
- A restorable tooth (adequate natural coronal tooth structure and clinical attachment levels, no vertical root fractures).
2. ‘Teeth with inadequate root canal filling when the coronal restoration requires replacement, or the coronal dental tissue is to be bleached’
The rationale for this technical indication is to prevent the ingress of bacteria or bleaching materials into the root canal system during the restorative intervention, the latter of which can result in the initiation of external root resorption.
Presenting symptoms
Patients attending a consultation for a root filled tooth will often present as follows:
- Asymptomatic with or without previous acute episode
- Symptomatology consistent of endodontic pain
- Symptomatology inconsistent with endodontic pain.
Orofacial pain of non-odontogenic origin (ie temporomandibular (TMJ) disorders secondary to myofascial pain, sinusitis, tension and vascular headaches, and neuropathies namely post-traumatic trigeminal neuropathic pain and persistent idiopathic dento-alveolar pain) commonly presents as tooth pain (Pigg et al, 2021). When the patient is or has previously experienced symptoms, it is thus imperative to confirm these are typical of endodontic pathology via a comprehensive pain history.
Features such as dull, throbbing, long lasting and well localised pain that has been successfully managed with over-the-counter analgesics or antimicrobials is a common presentation of root filled teeth with active periradicular disease.
In contrast, descriptions of pain such as numbness, tingling or burning sensations, or a failure of the initial root canal treatment and analgesics to successfully manage the pain, should raise suspicions of a non-odontogenic origin for the pain at a very early stage in the consultation and may warrant referral to an orofacial pain clinic in the absence of obvious clinical and/or radiographic findings.
Determine the outcome of the primary root canal filling
Subsequent clinical and radiographic examination should be systematic and focus on categorising the outcome of the primary root canal treatment into one of the following (ESE 2006):
- Favourable: Absence of pain, swelling and other symptoms, no sinus tract, no loss of function and radiological evidence of a normal periodontal ligament space around the root
- Unfavourable: The tooth is associated with signs and symptoms of infection. A radiologically visible lesion has appeared subsequent to treatment, or a pre-existing lesion has increased in size. A lesion has remained the same size or has only diminished in size during the four-year assessment period. Signs of continuing root resorption are present
- Uncertain: Radiographs reveal that a lesion has remained the same size or has only diminished in size.
It is worth noting that the above outcomes are independent of the technical quality of the existing root filling and unless an extensive coronal restoration or non-vital internal bleaching is to be provided, a poor-quality root filling in the absence of active periradicular pathology is not indication enough to proceed with endodontic retreatment.
Determining the most appropriate course of treatment
The above categories can be used to help determine the most appropriate course of treatment. For instance, a favourable outcome would indicate no further endodontic intervention.
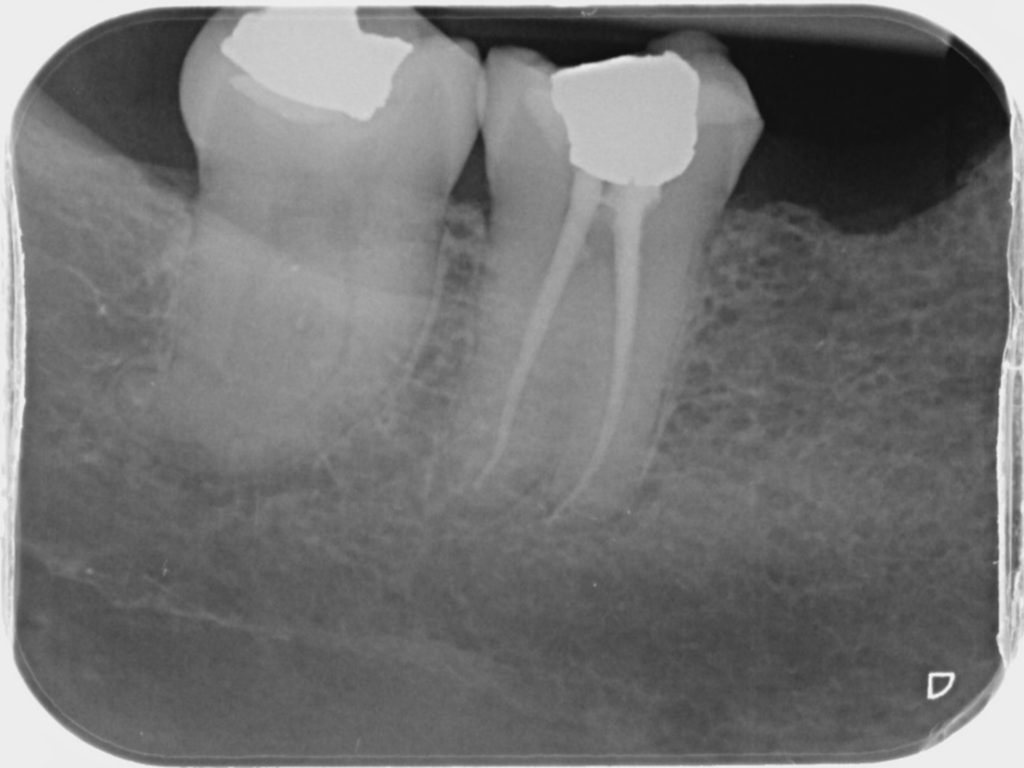
If, however, a patient is symptomatic in the absence of obvious clinical signs and symptoms from the tooth in question, further investigations such as a small field of view high resolution cone-beam CT examination alongside an actionable radiology report or referral to an oral-fascial pain clinic may be warranted to confirm diagnosis. It is important not to commence treatment prior to confirming a diagnosis so not to exacerbate patient symptoms, as can be the case for post-traumatic trigeminal neuropathic pain (Figure 1).
If the primary root canal filling is deemed to have an unfavourable outcome, then the next challenge is to ascertain the likely source of the pathology. For example, the driver for the endodontic pathology is likely to originate from within the root canal if no rubber dam was used, there is defective coronal seal, poor quality primary root filling or missed canals, all of which are amenable to non-surgical root canal retreatment.
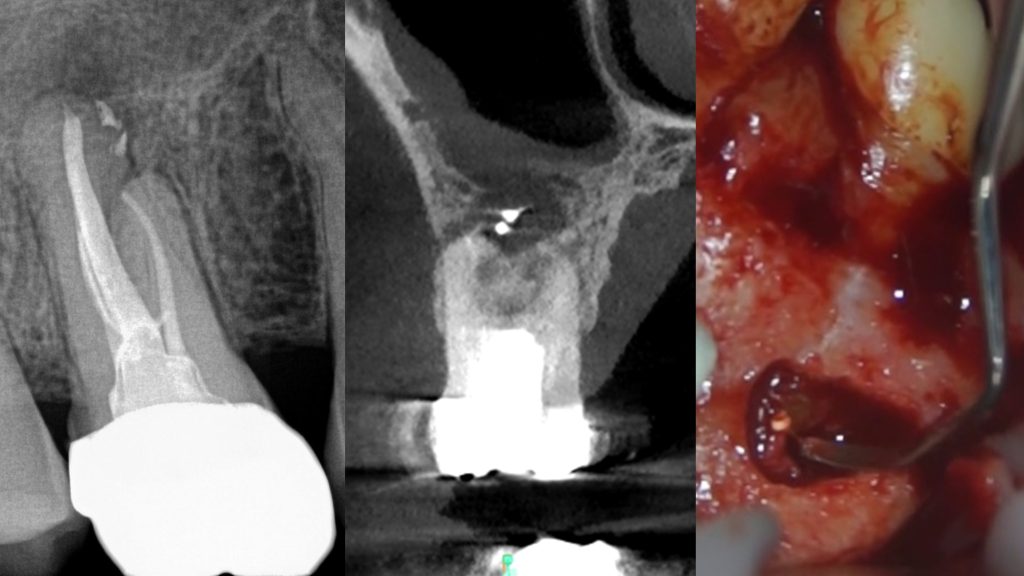
Conversely, persistent periradicular pathology in the presence of a guideline standard root canal treatment and coronal seal, foreign body reactions to extruded materials and self-sustaining cystic lesions are more amenable to an endodontic microsurgical approach (Figure 2).
In the presence of an uncertain outcome, continued annual clinical and radiographic monitoring of the tooth is indicated up to four years from the point of initial obturation. If within this period the radiographic lesion resolves, the outcome changes to favourable.
Conversely, if the tooth becomes symptomatic alongside clinical features, the radiographic lesion increases in size or only reduces in size over the four-year period, then the outcome changes to being unfavourable. The respective treatment pathways can then be offered to the patient.
Conclusion
It is hoped the above provides practitioners with guidance on when to and when not to endodontically retreat and introduces them to the subtle nuances in these types of cases that would warrant further investigations.
Email [email protected] for references.
Catch up with the Endodontics 101 series:
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

