
Michael Heffernan discusses the different reasons patients seek overseas treatment, and the risks and complications they should be informed about.
I originally set out this article to highlight the true costs for patients returning from having cosmetic dentistry overseas. But I realise this is also relevant to the decisions we make in clinics in the UK too.
Cosmetic dentistry is on the rise, fuelled by the appreciation that an attractive smile can improve a person’s self-esteem, personal life and even career. Social media and influencers also drive the quick-fix ‘restorative’ remedy to less than perfect teeth.
Why would you wait?
However, the decision on how to improve the appearance of our smile carries a number of factors:
Time – we hate to wait
Because of immediate results, we have seen patients that have travelled overseas to dental clinics and returned with 24 teeth being fitted with full coverage crowns. This is to give the appearance of straight (super) white teeth.
However, to overcome irregular tooth positions, the crown preparations can be extensive. Often the patients are young with large pulps and the pre-operative pictures show minimal previous restorative treatment. Therefore, the preparations are incredibly damaging to the teeth.
Sadly, ‘minimally invasive’ approaches would often have been possible but they typically would have taken longer to complete so are not suited to a flying visit.
Cost – now versus ultimate cost
Patients often think of the cost of the procedure to make the beautiful smile as simply that on the quote at the time of treatment.
However, the more complex the dentistry and the more teeth involved, the more the ongoing costs will be as no restoration lasts forever. It is likely hard for a patient at the time of consenting to treatment to imagine the longer-term costs of that treatment approach.
Maintenance – new restorations are in a very harsh environment
All dental treatments carry a risk of failure. Poor quality dentistry can create niches for bacteria to inhabit, increasing the risk of caries, periodontitis, pain, infection, halitosis and even chronic ill health through inflammatory disease processes.
The ability of the patient to be able to look after the new restorations with good oral hygiene will determine the longevity of the restorations.
The concept of ‘minimal intervention’ dentistry is the approach recommended in UK dental schools and has been adopted by the chief dental officer of England.
The belief is to preserve as much of the natural teeth as possible as enamel/dentine are generally superior to any artificial restoration, and the more natural tooth preserved will increase the success of a subsequent restoration; the greater the damage to the tooth the shorter the lifespan of that tooth.
Hence the ideal approach to get white teeth and a stunning smile without the heartache could include:
- Tooth whitening – with well-fitting trays and a legitimate tooth whitening kit
- Orthodontics – when your teeth are in the right place, smaller composite bonding restorations can be more easily carried out and there is less risk of crowns/veneers debonding
- Composite bonding – to build up worn, discoloured or chipped/eroded teeth. This is usually an additive process that minimises the tooth reduction and therefore damage to pulp and tooth.
Real costs of ‘maximum invasive’ treatment approach
Let’s take an example of a recent patient to understand the differences in the above approaches. This person had all their teeth crowned in a clinic abroad.
They could have had orthodontic treatment to upright and align the front teeth with tooth whitening and composite bonding to make up for the deficient/ wear facets.
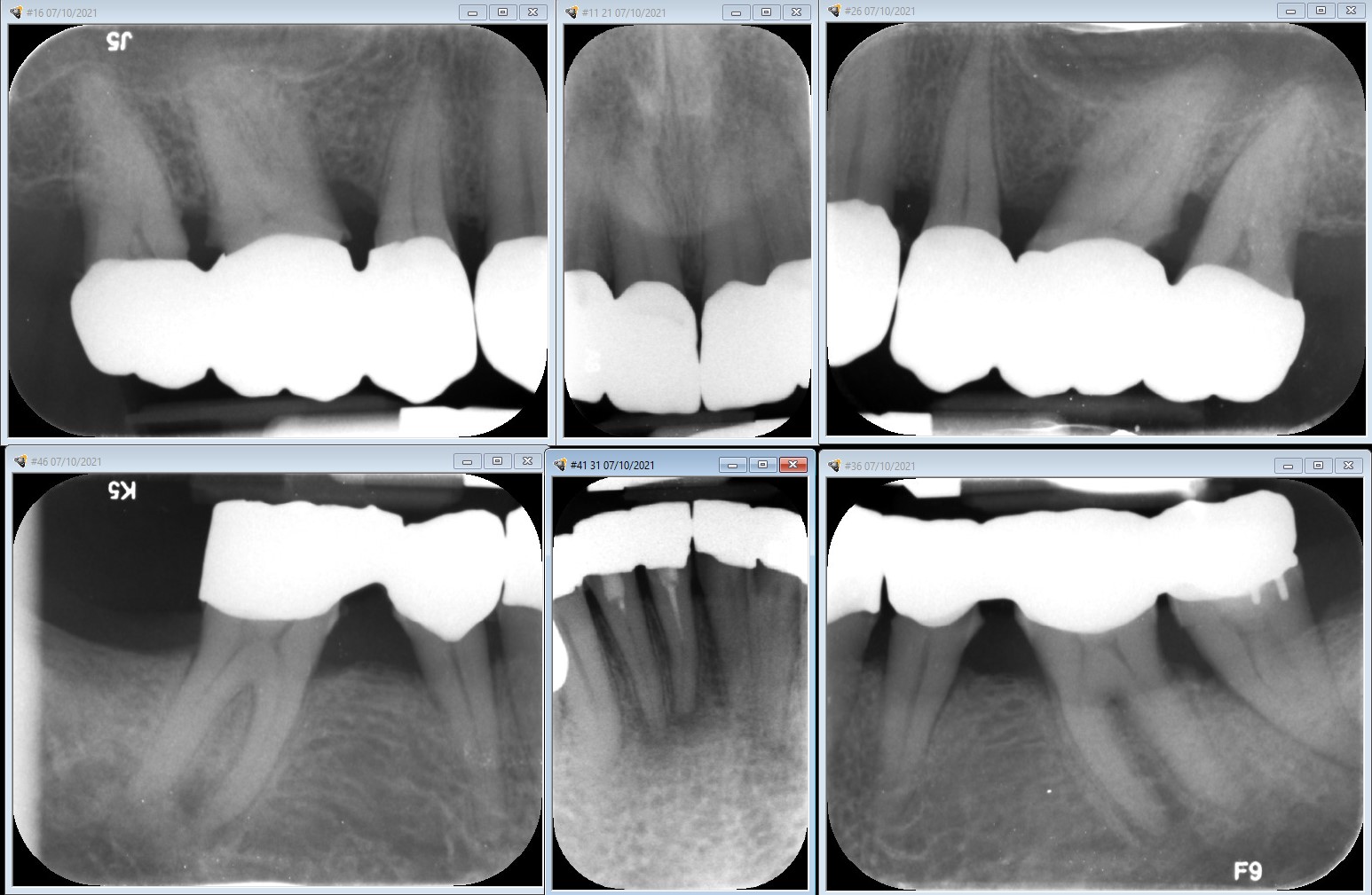
The crowns fitted abroad were all joined together so they were impossible to clean (figure 1). They also both had deficient margins leading to sensitivity or large ledges causing the gingiva to become inflamed and bleed.

If we consider the real costs for this patient, we need to factor in the cost to have the work and add the long term costs. Every restoration that is cemented has a certain amount of time that it will cope with the rigours of the mouth. In a typical person the longevity of a crown is approximately 10 to 15 years.
Hence when we consider the quick-fix restorative approach to improve the smile of this man getting their front 12 teeth crowned, they will need to replace the 12 crowns four or five times in their lifetime compared with zero crowns. In addition, just composite could have been considered in this case.
Replacing and amending work
To work out the true costs of these different treatment approaches, we can look to the Judicial College Guidelines which provide figures for certain injuries. While the guidelines do not provide specific information on the lifetime costs of crowning a tooth, they do provide a range of compensation amounts for replacement of two front teeth. This is dependent on the severity of the injury and the treatment required.
The compensation amounts range from £5,200 for a simple replacement of two front teeth to £30,000 for more severe injuries that require more extensive treatment, such as dental implants or bone grafting.
It is important to note that these compensation amounts are intended to cover not only the cost of the dental treatment but also any other related costs, such as travel expenses, loss of income and pain and suffering. Additionally, the compensation amounts in the Judicial College Guidelines are intended as a general guide and may vary depending on the specific circumstances of each case.
To get a longterm cost for the twelve front teeth, let us take the conservative number of £5,200 for ‘two front teeth’ from the Judicial College Guidelines and multiply this by six (12 teeth).
Therefore, the cost for replacement of the twelve front teeth over a lifetime might easily be £31,200 to try and amend/maintain work that did not need to be done in the first place. Even this does not quantify the reality of prosthetic teeth instead of their real natural original teeth with good proprioception and predictability.
Biological costs
Beyond the financial costs, there are biological costs to extensive crown preparations compared with veneers or composite bonding. If we consider the dental ramifications of a crown versus a veneer (where minimal or no tooth is removed) there are large differences in the tooth outcomes.
To judge what these may look like, the best evidence is from a large data set of more than three million patients by Lucarotti and Burke (2018) carried out in the UK. The outcomes of note are:
- Approximately 20% of teeth that are crowned will need root canal treatment in five to 10 years
- At 15 years, 25% of crowned front teeth will have been extracted compared with only 7% of veneered teeth. The extracted front teeth will then need to be replaced with implants, bridges or dentures
- Crowning an incisor tooth will lead to an earlier time of extraction. The younger the patient, the greater the risk when compared to veneers or composite bonding
- Even veneers, which are used to improve the appearance of teeth, have a high failure rate with almost 60% lost at 15 years albeit that the tooth is still present to restore again
- Only 35% of restorations survived without further intervention at 15 years. Many patients do not recognise that dental restorations have a limited lifespan.
Avoidable dental work
If we return to the ‘typical’ dental tourist that we see in our clinic – a 20-30-year-old with relatively good teeth – by time they are 45 years old, of the 12 front teeth unnecessarily crowned, they will have seen three of them needing root canal treatment and the three front teeth extracted.
Only four of the original crowns will still be in place without intervention or replacement/removal with lifetime costs today of at least £31,200 (beyond the cost of going for the treatment overseas in the first place).



Minimal invasive dentistry approach
With this approach we try and avoid damaging the teeth by repairing erosion and tooth caries by remineralisation agents such as fluoride or calcium phosphate.
This was the reason behind us inventing Dr Heff’s Remarkable Mints, which contain xylitol, green tea extract and calcium phosphate, to help repair teeth on-the-go.
However, when teeth are damaged beyond the scope of us remineralising the surface, we will need to intervene. Typically we prefer using composite bonding for front teeth.
The advantage to this is maintaining the longevity of the tooth by bonding directly to the enamel rather than reducing the tooth with a dental handpiece. The risks are that the material may need to be repaired/replaced over time or re-polished if there is significant staining.
The annual failure rates vary from zero to 4.1% for anterior composites. However, these restorations can be carried out in a single sitting with immediate beautiful results without the many other compromises from crowns.

Summary
Anyone considering travelling overseas for cosmetic dentistry needs to be clear of the risks and extensive biologic and financial costs of ongoing care.
Patients should be made clear of what type of restoration they will be receiving and have a real gauge of the quality of the work, rather than judging the outcome on appearance or recommendations of poorly qualified ‘influencers’.
For references, please contact [email protected]
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

