 What can labs do to combat same day milled in practice prostheses, that are cutting out the key middle man?
What can labs do to combat same day milled in practice prostheses, that are cutting out the key middle man?
‘Provocative’ is my first suggested blog.
We have all seen the seismic change in digital manufacturing in the dental laboratory. Nobody would now suggest we take it away. It has become an essential tool in designing and manufacturing. It extends our range, it can improve quality, make life easier, reduce the drudgery of some tasks, improve efficiency, more profitable… Well, you get my point; there is no turning back.
The introduction of in-surgery digital scanning has been relatively slow and digital milling is still quite rare. Of course, dentists only usually spend money to make more money, so this is probably a clue to the low rate of uptake.
Milling statistics
Laboratories save on time and salaries. Whereas for the dentist it is another role to take on and they can make much more money doing clinical work than laboratory work.
I have concentrated on fixed restorations. I think we are still some way off manufacturing prosthetics in surgery.
It is difficult to obtain statistics, but understand that the percentage of surgeries with digital scanners for impressions is coming up to the 10% mark. And the percentage with milling equipment not yet 5%.
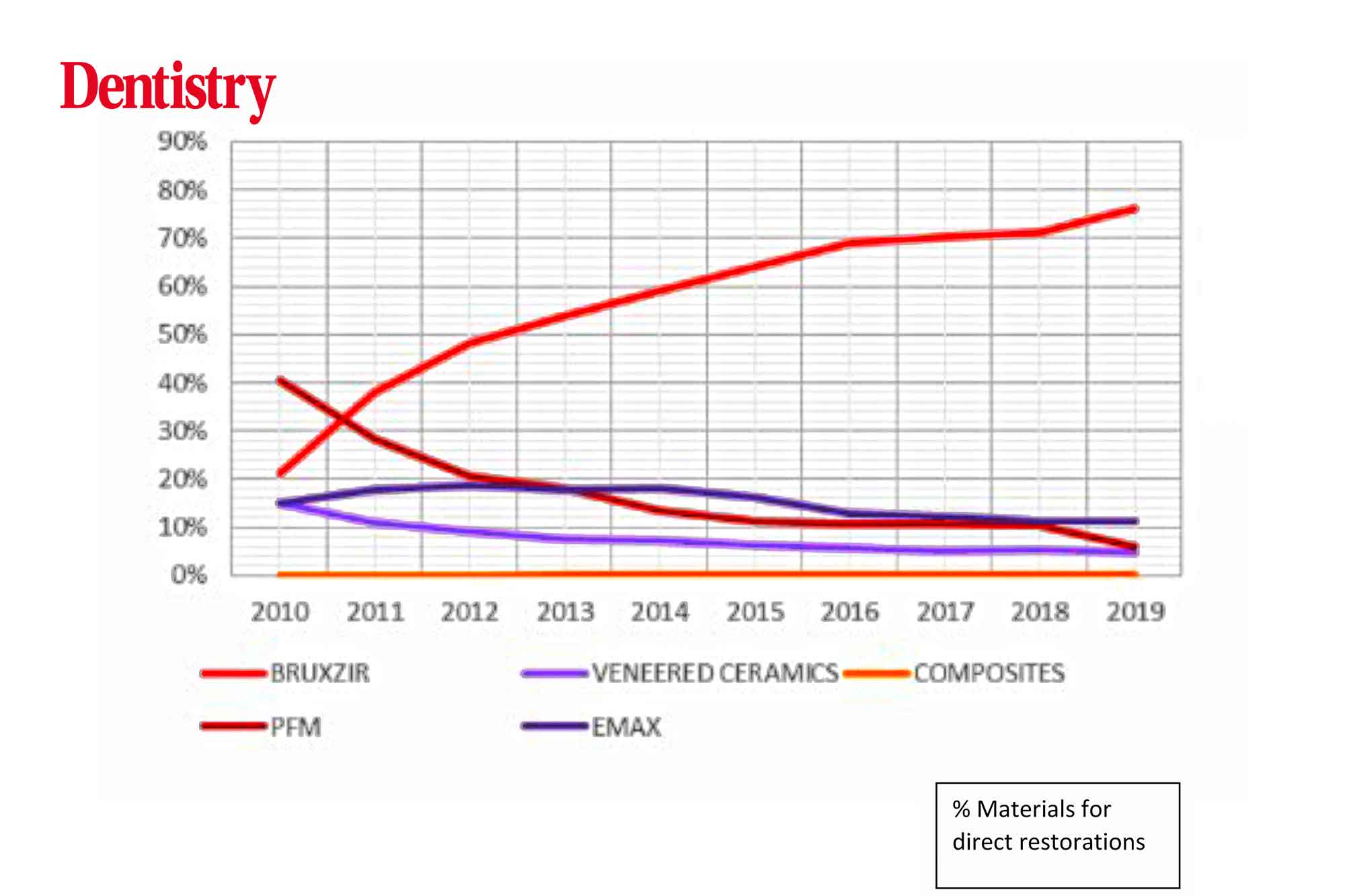
My colleagues in the USA tell me that PFMs are down to about 9% of restorations and bruxir (monolithic zirconia) up to 75% of all cases. Glidewell predicts that by 2025 over 80% will be laboratory-manufactured from monolithic zirconia (Figure 1).
Yet surprisingly, in the US the number of surgeries in-house milling is very low (8.79%).
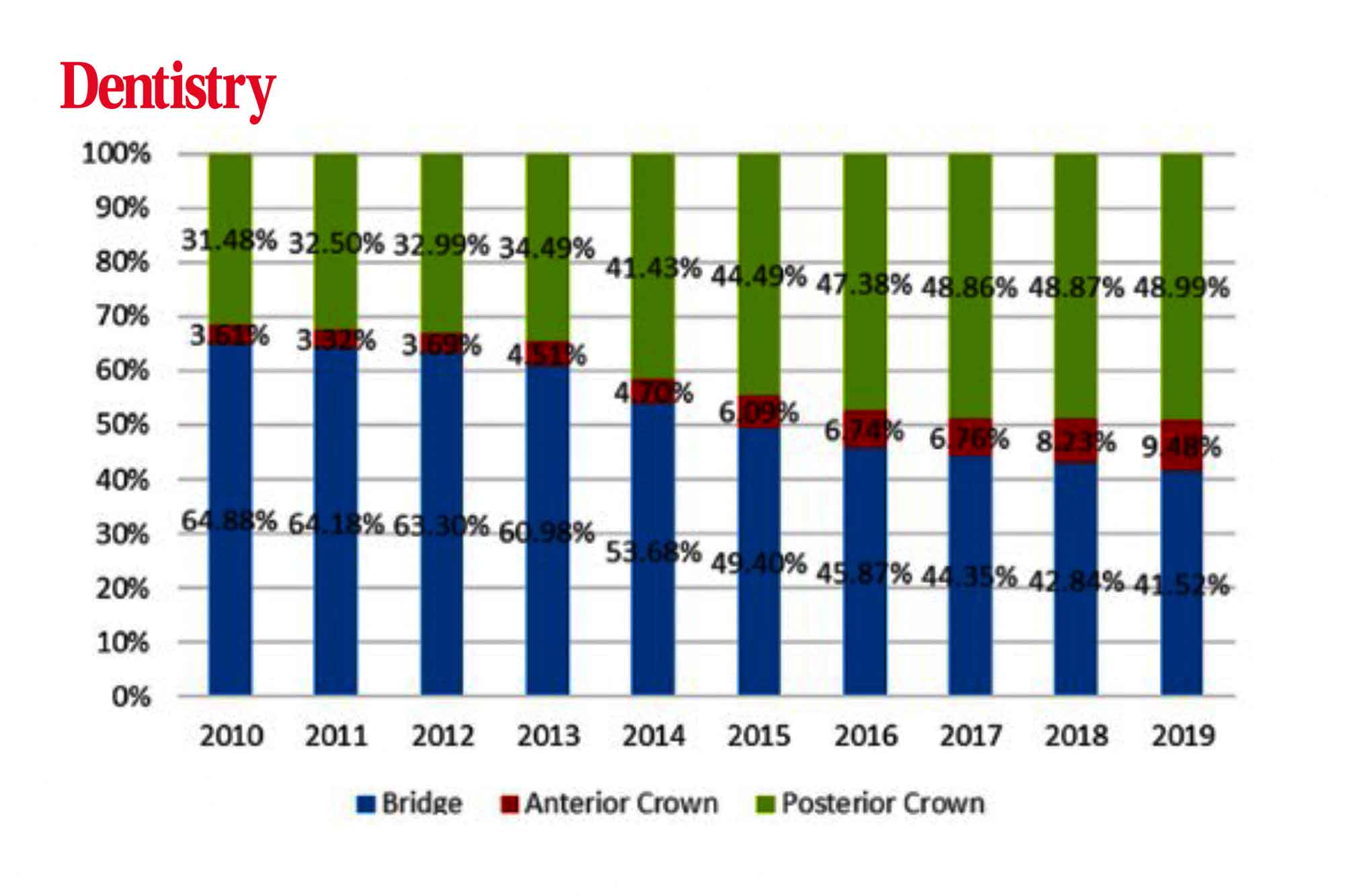
Interestingly the types of restoration manufactured by in-house systems has changed significantly. The number of bridges is reducing and single posterior crowns rising. Posteriors up from 31% to 49%, bridges 65% to 41% (Figure 2).
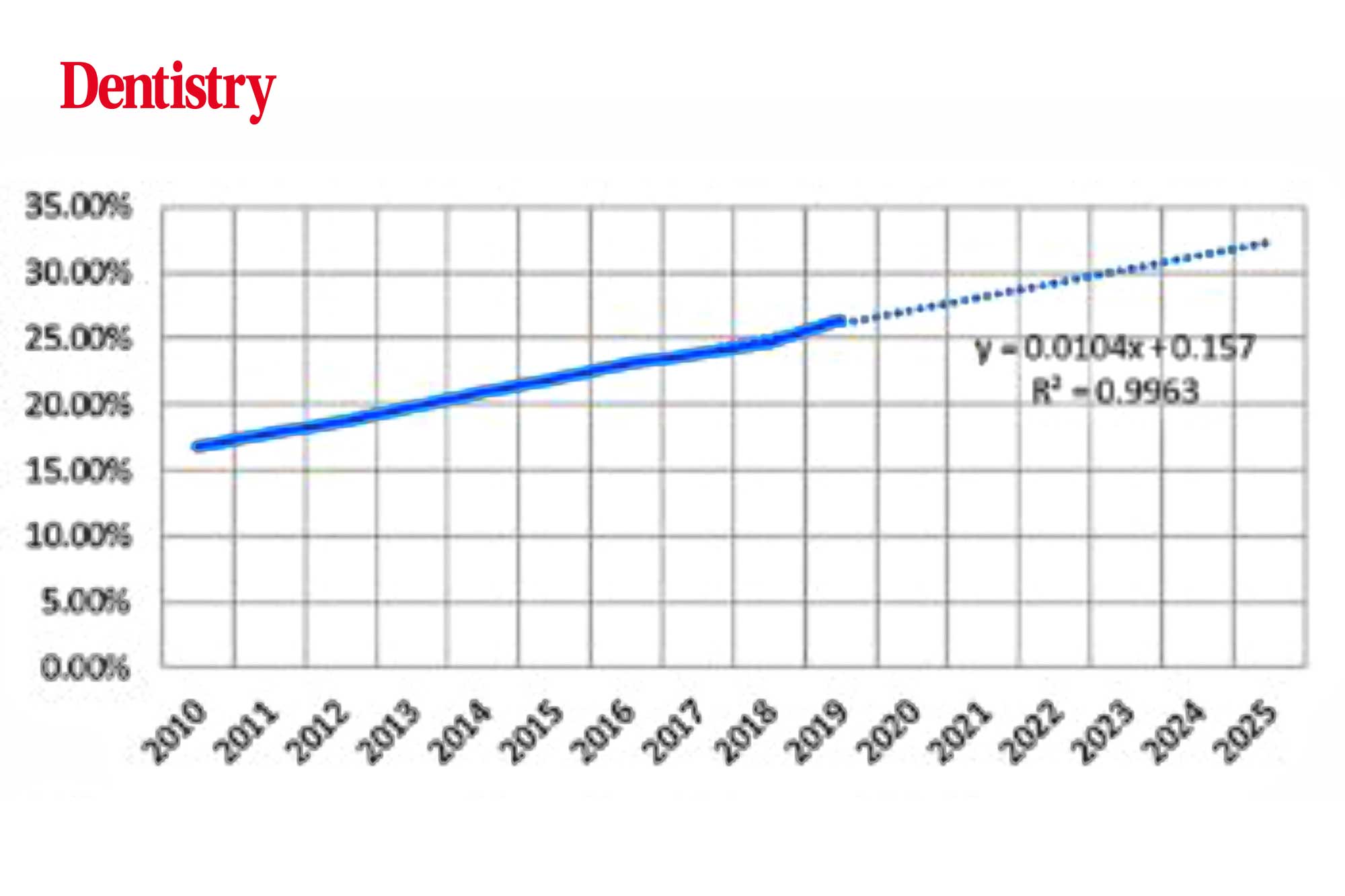
The number of dentists, who own scanners in the US sending work to Glidewell has risen over the last decade. So there is little sign of loss of work to in house milling (Figure 3).
Same day crowns
A discussion with some UK lab owners gave me the impression we have little to worry about in-house manufacture. The quality and aesthetic outcomes of anterior restorations is a long way from laboratory-manufactured restorations.
I believe the future of monolithic restorations is assured with it overtaking most materials currently in use. We can now mill monolithic zirconia crowns in the clinic delivering single visit crowns with a high polished appearance and excellent surface quality.
There is a place for same day in-house surgery manufactured crowns. But I believe it will play a small part in the overall picture.
One issue in this, of course, is the number of technicians in the UK to manufacture this work.
In my next blog I will have a look at how the laboratory industry can manage the surge in work when the UDA requirements change in September.
My thanks to an article by David Leeson at Glidewell Dental Newport, CA USA for the statistics and graphs in Elsevier Health Journal.

