
Isaac Tawil, Scott Ganz and Michael Erdos investigate the digital management of functional occlusion utilising digital pressure-sensing registration.
Abstract
The primary goal in the treatment of patients with full-arch restorations is to ensure a comfortable, functional occlusion with a structurally sound restorative prosthesis. While prosthetic failure is a multifactorial issue, occlusal overload is an important potential contributing factor.
Until recently, intraoral occlusal measurement has been confined to the use of articulation paper. However, occlusal measurement technologies have now advanced to include the use of digital occlusal-pressure articulation, which allows the recording of masticatory forces over a designated time period. OccluSense (Bausch – Köln, Germany), a wireless digital device for occlusal pressure measurement, combines traditional carbon articulation with digital pressure-sensing registration to enable clinicians to view occlusal pressure patterns and evaluate premature or hyperocclusal contacts for potential reduction.
This article provides a case study comparing traditional articulation versus digital occlusal-pressure articulation using the OccluSense digital device, both of which were used in a patient who required full-mouth rehabilitation.
Introduction
The use of full-arch implant-supported fixed restorations in clinical practice has increased dramatically over the past several decades.
At the same time, patients today have a greater awareness of the various full-arch implant options that are available, as well as the potential financing and payment plans for treatment, and thus are better empowered to enhance their quality of life through the improved function and aesthetics of restored dentition.
As a result, dental occlusion has once again become a highly relevant and important topic in dentistry, as ensuring a functional occlusion is central to successful full-arch rehabilitations with a structurally sound prosthesis.
Role of occlusion in prosthetic failure
For decades, conventional crown and bridge dentistry for both natural teeth and dental implants has been achieved with ceramo-metal restorations. While metal has always served as a reliable substructure that is highly resistant to fracture, the secondary ceramic layers have been prone to chipping or fracturing as a result of misdirected or excessive occlusal forces.
Improvements in ceramic materials (eg, zirconia) and production capabilities (eg 3D printing, milling units) have been helpful in enabling laboratories and dental technicians to fabricate stronger, longer-lasting solutions.
In addition, improved synergies between ancillary technologies such as intraoral scanning, photogrammetry, and virtual articulation have reduced the production time and increased the accuracy of ceramo-metal restorations.
However, even with stronger and more precise ceramic materials, prosthetic fracture and implant failure due to occlusal overload remain a valid concern.
Prosthetic failure is a multifactorial problem that goes beyond issues of ceramic strength. One factor that contributes to potential restorative failure is increased stress due to lack of appreciation of the proper vertical dimension of occlusion (VDO). Another is reduced height and thickness of material, or poor reduction of substructures. Also, increased cantilever or pontic lengths due to poor anterior- posterior spread (A-P spread), or an unbalanced occlusion.
An occlusal high spot on a screw- retained prosthetic in the location of a titanium base (ti-base) often results in fracture propagation, as it is a point of weakness (Figure 1).

Advancements in occlusal measurement technologies
Dental occlusion has been studied for decades, resulting in various schools of thought regarding optimal treatment. While the 3D relationship of the jaws is clearly defined by the VDO, horizontal centric relation, and envelope of function, theories regarding occlusion may conflict as to whether occlusal function is tooth-borne, neuromuscular, skeletal, static, dynamic, based on centric relation, or based on centric occlusion.
Regardless of differing opinions, the common goal in the treatment of patients with full-arch restorations is to ensure a comfortable, functional occlusion with a structurally sound restorative prosthesis, which will ultimately result in improved patient satisfaction.
While dental technology has progressed dramatically over the past several years, until recently traditional measurements of occlusal contacts and balance have undergone very little change.
Although extraoral articulation is extremely valuable and has been enhanced through the use of digital technology, conventional measurements of intraoral occlusion have remained limited to the use of articulation paper (Figure 2), the clinician’s observations of carbon paper markings, and the patient’s awareness of pressure.
Benefits of occlusal measurement technologies
Unfortunately, patient perception becomes increasingly difficult to utilise when proprioception is absent or diminished, as is the case with patients who have dental implants. In patients with full-arch and full-mouth implant rehabilitation, a broader awareness of the patient is required, with muscular and skeletal sensations utilised to convey potential occlusal imbalances that are otherwise often unnoticed.
Initially, intraoral occlusal measurement technologies could be used only to measure static pressure points through the use of gauges. Over the past few years, however, these technologies have advanced to include digital devices that can capture pressure and movement over time, thus greatly enhancing diagnostic competencies.
By incorporating these innovative technologies with traditional methods, clinicians can achieve an ideal measurable outcome, which in turn will improve the functionality and resiliency of both temporary and final restorative materials.
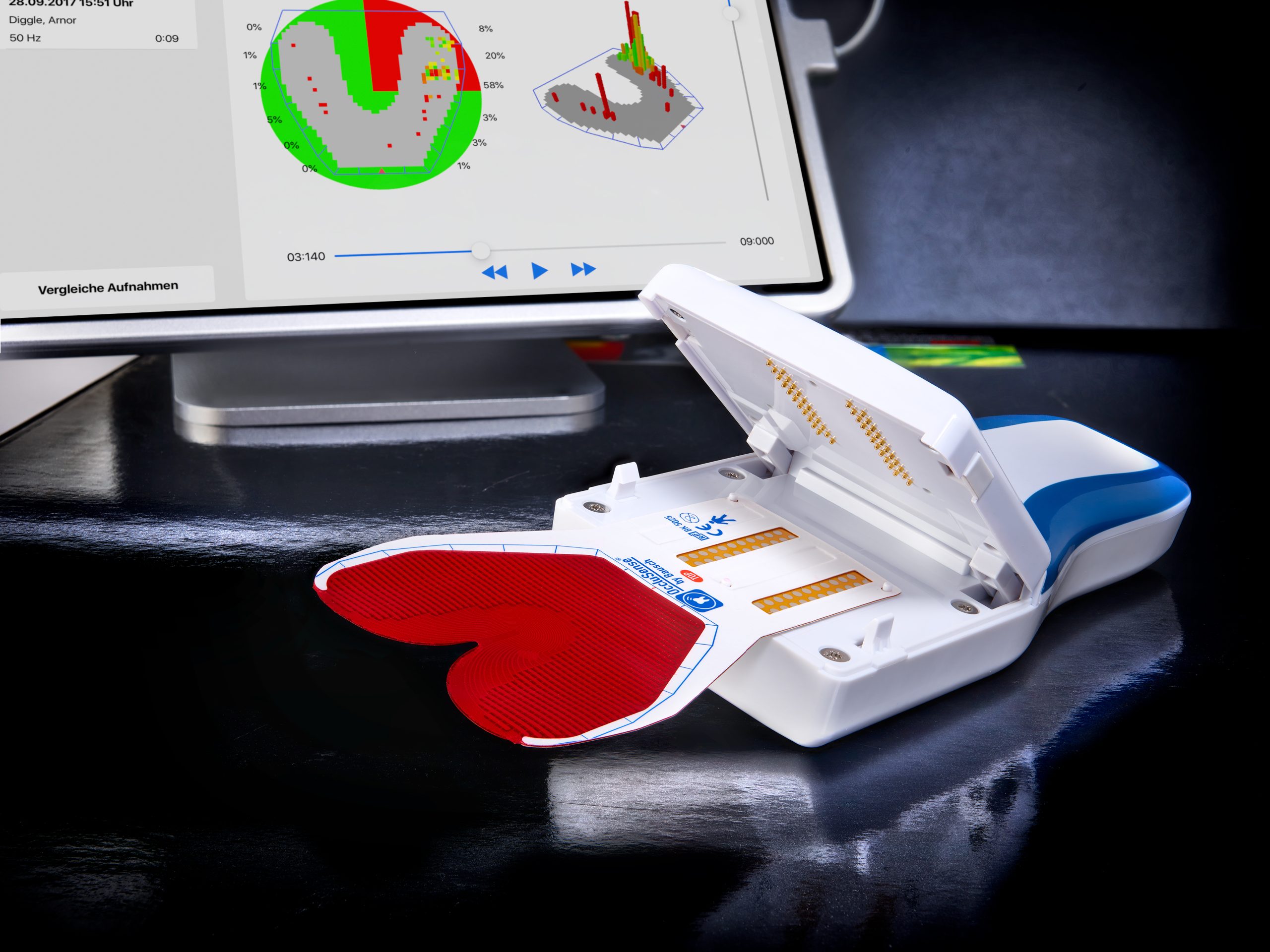
An innovative wireless device called OccluSense (Bausch – Köln, Germany) combines traditional carbon articulation with digital pressure-sensing registration, allowing the recording of masticatory forces over a designated time period (Figure 3).
How does OccluSense work?
A disposable, 60-micron thin, red, carbon-lined pressure sensor is inserted into the device and applied in the manner of traditional articulation foil. The masticatory pressure is recorded digitally with more than 1000 points of contact in 256 pressure levels and is transmitted wirelessly to an iPad. The device has the capability of capturing both static and dynamic occlusion.
The captured data can then be viewed as 2D and 3D graphics, with up to 150 images recorded per second. The recordings can be measured over a selected period of time. In ‘live’ mode, the duration is not limited, while in ‘recording’ mode, a set time is needed to conclude the data collection. The recordings can collect temporal progression data, from the initial contact to the final intercuspal position in maximum intercuspation.
Once the transfer is completed, the clinician can utilise the OccluSense software to view the occlusal pressure patterns and evaluate premature or hyperocclusal contacts for potential reduction. Multiple occlusal sessions can be recorded for the same patient until a desired occlusal result is achieved.
Indications for OccluSense
Indications for digital occlusal-pressure articulation include, but are not limited to, pre- and post-orthodontic movements, temporomandibular joint dysfunction (TMD), and restorative dentistry procedures ranging from simple single-tooth restoration to full-mouth therapy.
The authors recommend that the device should be used in conjunction with traditional methods to provide the highest level of accuracy in the measurement of functional occlusal relationships.
The following case presentation compares the use of traditional articulation versus digital occlusal-pressure articulation using the OccluSense digital device, both of which were used in the same patient to aid in the recording of premature and eccentric contacts and to decipher occlusal patterns for the facilitation of accurate full-mouth rehabilitation.
If you would like to read further, visit www.occlusense.com/article-tawil.

