
We hear from a number of experts about how the G-ænial Universal Injectable adds an unrivalled level of reliability and predictability to their treatments.
Injection moulding technique with injectable composites: quick fix or long-lasting solution?
The injection moulding technique with injectable composites, which became known to dentists worldwide due to the work of Dr Douglas Terry, has become increasingly popular in the latest years.
It is a relatively simple procedure that makes it possible to obtain a predicable end result, even in complex situations, because the morphology can be determined in advance.
It is in part because of the development of suitable, high quality materials, such as G-ænial Universal Injectable and Exaclear that injection moulding is a reliable procedure.
G-ænial Universal Injectable has the ideal consistency and mechanical properties and thus it is widely used for this technique.
Combined with the highly transparent Exaclear silicone, the technique has become approachable and easy to conduct. In the following overview, it is shown how the restorations that were made with this technique can stand the test of time.
Case 1: Restored occlusion after severe general wear by Professor Marleen Peumans, Belgium
Because of its high wear resistance, G-ænial Universal Injectable can also be used to restore occlusal surfaces. This is particularly useful in case of abrasion/erosions in the molar area and has the advantage that it can be used in a minimally invasive way.
In these cases, careful planning is imperative to restore the function in a correct manner. Injection moulding is a valuable method for a correct restoration of a physiologic occlusion with the aid of digital modelling techniques.
Two models were printed: one with every second tooth restored and another one with all teeth restored. Based on those, two transparent silicon indices were made (Exaclear, GC).
Working with two silicone indices has the advantage that the intraoral seating is more stable, there is greater control of excess material on adjacent teeth and a better emergence profile can be created.
Four models were made in total (two per jaw). One year after treatment, the surfaces still look smooth and shiny, without obvious occlusal wear facets.


Figure 1A: Worn occlusal surfaces and maxillary diastema before treatment. The colour of the teeth, discloses the loss of surface enamel, with the colour of the dentine clearly showing through .
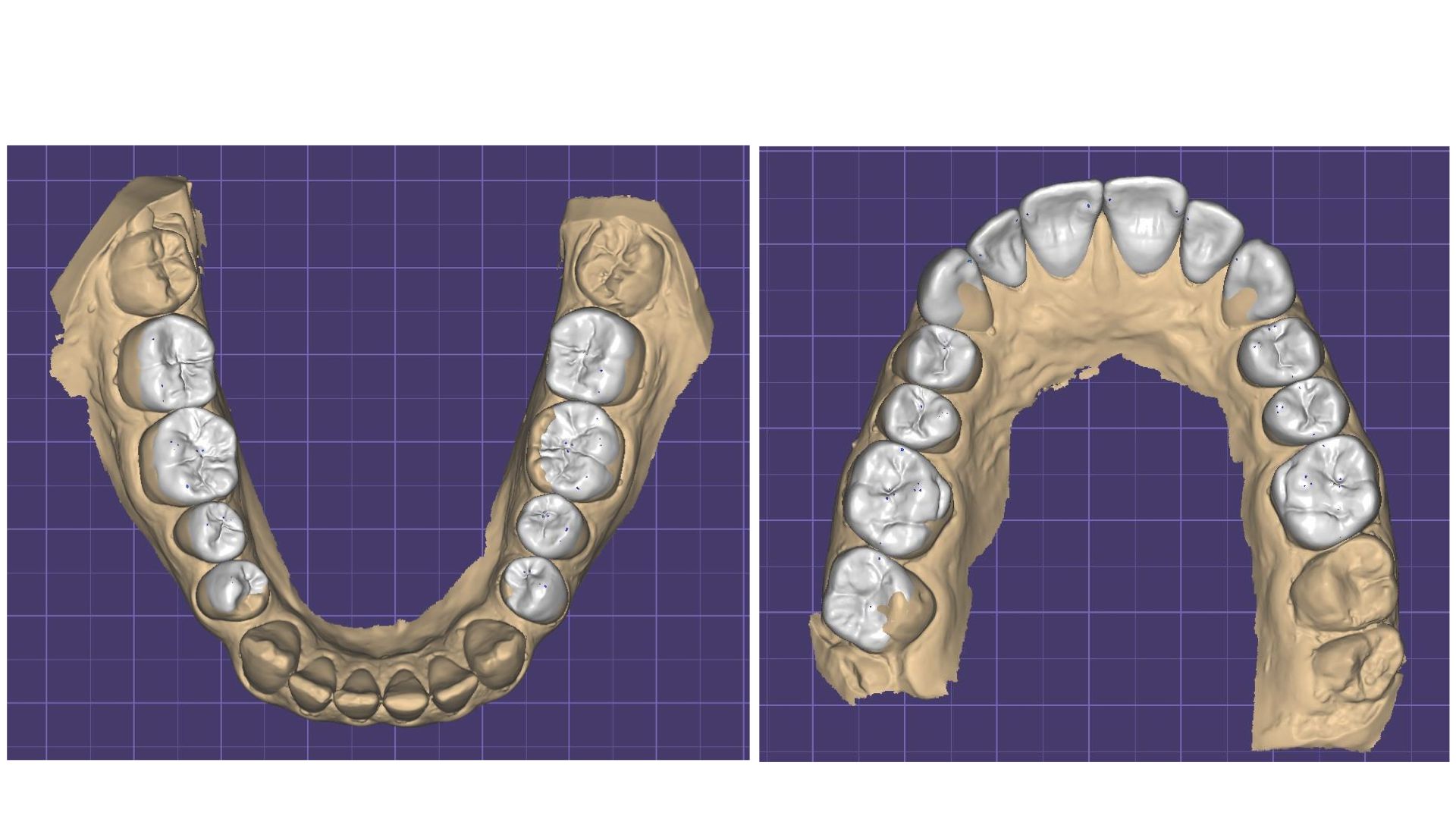
Figure 1B: Computer-aided design of the restored occlusion. The diastemata between the maxillary incisors were restored as well.
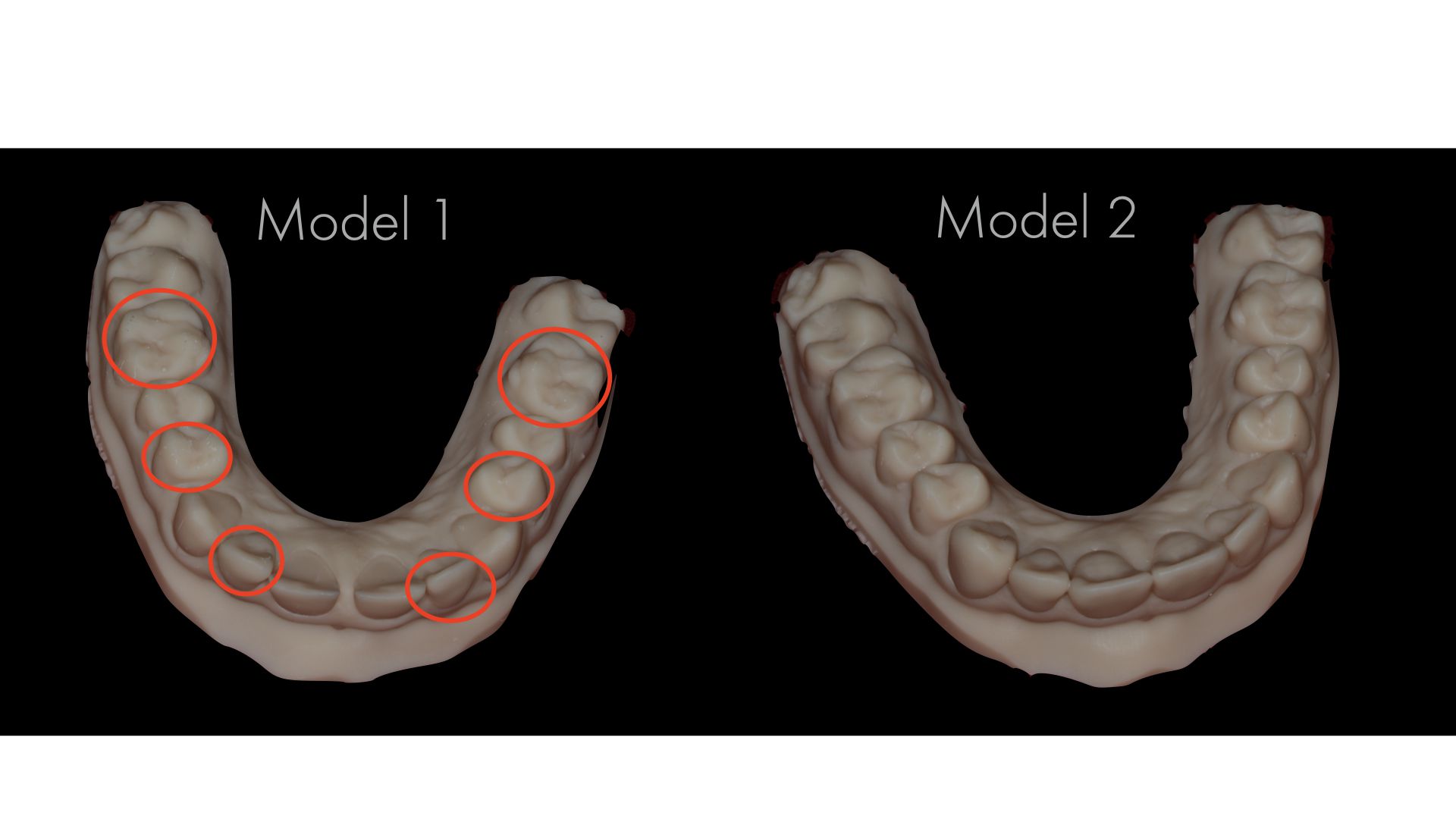
Figure 1C: The two 3D-printed models of the maxilla; in model 1, every other tooth was restored, while in model 2, all teeth were restored.

Fig. 1D: Injection moulding with G-ænial Universal Injectable in a transparent mould.

Figure 1E: Restored dentition after treatment.


Figure 1F: Close-up of the fourth quadrant. Top: before treatment; Middle: at baseline (after restoration); Bottom: one year after treatment.
Case 2: Cost-effective aesthetic rehabilitation by Dr David Geštakovski, Croatia
In the presented case, six composite veneers were made on the upper incisors and canines with the injectable moulding technique.
After facial analysis, teeth were scanned and a digital ‘wax up’ was made.
Based on the wax up, an intraoral mock-up was done to check guidance, functional parameters, aesthetics, and phonics. To get long lasting results, function needs to be planned in a correct way.
Therefore, canines were included to obtain canine guidance in order to avoid potentially harmful contacts and forces on incisors, which may cause chipping of the restorations. Because of the low lip line the patient’s gingiva was not visible in the forced smile so the asymmetry in the soft tissue around the central incisors was left as before.
In this case, the silicone indices (Exaclear) were again based on two different 3D-printed models, for the same reasons as mentioned in case 1 (vide supra).
Teeth were cleaned and etched, retraction cords were packed in the sulci to prevent crevicular fluid from flowing in field of work and to avoid subgingival flow of the injectable composite.
Adjacent teeth were isolated with Teflon tape and after the adhesive protocol (G-Premio BOND, GC), G-aenial Universal Injectable (GC) was injected and polymerised directly onto the teeth.
A1 shade was used for the incisors, while the canines were done with A2. For finishing and polishing, a scalpel no. 12, Epitex strips (GC), a fine diamond polishing bur and silicone spirals were used.
Two years later, the restorations maintained high aesthetic quality, without chipping or marginal discolorations.
The beauty of this technique is its predictability and possibility to achieve great symmetry and marvellous primary, secondary, and tertiary morphology.


Figure 2A: Initial situation.

Figure 2B: Checking the size of the injection holes in the silicon index (EXACLEAR, GC) on the first 3D-printed model.


Figure 2C: Result directly after treatment, showing nice shape and morphology. The gingival line was not modified since it was not visible during smiling.

Figure 2D: Result after two years. The shape of the restorations was maintained, without chipping or marginal staining.
Case 3: Interceptive restorative treatment of a full mandibular arch by Dr. Jacopo Mattiussi, Italy
In this case, G-ænial Universal Injectable was used to offer the patient a long-term temporary solution that did not hinder a more complex full-mouth rehabilitation in the future because the economic situation of the patient did not allow such treatment at the moment.
In contrast to the previous cases, no CAD/CAM technique was used to make the design, but a traditional wax-up and bite registration were done.
The vertical dimension was slightly increased and occlusal planes and curves were regularised as much as the pre-existing situation allowed it.
Here, only one clear silicone key was used to restore the entire lower arch was restored in a single session. The result impresses in terms of aesthetics and the patient was very satisfied. It was ensured that the patient could clean all interdental spaces and at follow-up, healthy gingival tissues could be seen.


Figure 3A: Initial situation. The upper jaw was restored three years ago by means of a voluminous zirconia full-arch restoration of which the patient was not very satified. The lower jaw was highly chromatic in comparison, with a considerable amount of tartar, extensive destruction of the hard tissues and periodontal attachment loss.


Figure 3B: Impression taking and facebow registration. The wax-up was made with the aim of increasing the DVO just enough to regularise the occlusal planes and curves, with obvious limitations dictated by the morphology of the upper maxillary rehabilitation.

Figure 3C: The lower are was restored per sextant. Old restorations were removed, cavity edges rounded and their surfaces sandblasted. The enamel was selectively etched before application of G-Premio Bond(GC).



Figure 3D: Images taken two and a half months after treatment. Harmonised aesthetics, a normalised vertical dimension and excellent health of the soft tissues are evident from the observation.
Case 4: Treatment of localised wear of anterior teeth by Dr Kostas Karagiannopoulos, United Kingdom
A 45-year-old man presented complaining of the appearance of his front teeth. Severe localised tooth surface loss of multifactorial origin led to short clinical crowns.
Worn teeth in occlusion due to dentoalveolar compensation have the restorative disadvantage of lack of interocclusal space.
It was decided to proceed with additive composite restorations to restore the affected teeth using the Dahl concept: this is a method of treating the localised wear of anterior teeth, without having to treat the posterior teeth. The latter are discluded and allowed to re-establish itself over time.
All primary disease was controlled prior to the restorative phase, including the intrinsic acid erosion.
Alternate technique
The alternate tooth technique was used to carry out the injection moulding technique. Once proximal and gingival excess was removed on all six restorations there was minimal finishing as the anatomy was wax-up driven and not freehand.
The final result exhibited good surface texture and lustre whilst anterior guidance was maintained.
At a follow-up appointment after 20 months, no chips, fractures or debondings were observed. The patient is a heavy smoker and sees the hygienist regularly.
Occlusal contacts were fully re-established on the posterior teeth after completion of the Dahl movements and the patient is now wearing an occlusal appliance at nights. Of note is the high gloss retention of the six direct composite restorations.
No further polishing was done on the facial surfaces during that 20 month period.

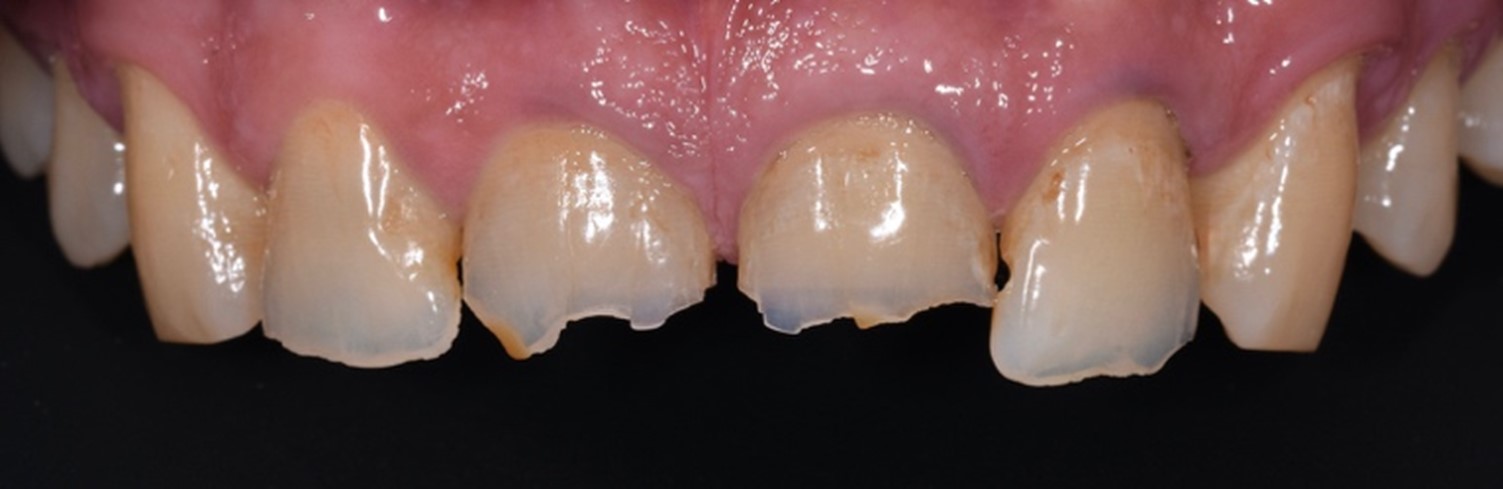


Figure 4A: Pre-operative photographs.

Figure 4B: Diagnostic wax-up on printed models.




Figure 4C: Immediate treatment result. The ability to replicate anatomic details and microtexture on the facial surface with the injection moulding technique combined with a fairly rigid stent exceeds that of all other direct composite techniques. Note the slight disclusion in the posterior area.

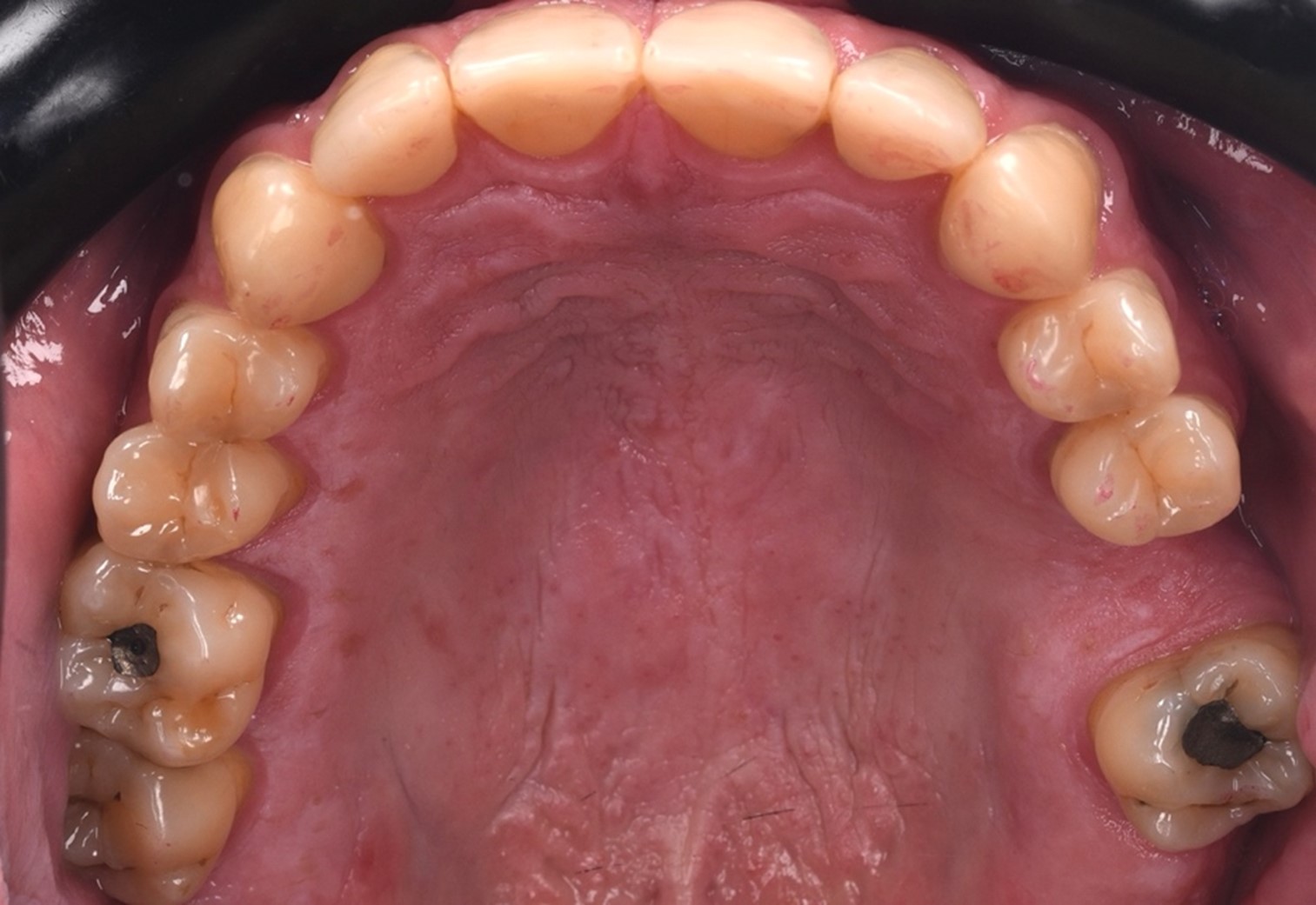

Figure 4D: At the 20-month follow-up, the occlusion was fully re-established. The high gloss retention of the six direct composite restorations was noteworthy, eliminating the need for repolishing.
Conclusion
Injection moulding has a wide range of indications, from anterior to posterior, from interceptive to final restorations, for aesthetic as well as functional rehabilitations, without excessive requirements in terms of clinical skills.
The excellent strength and gloss retention of G-ænial Universal Injectable contribute to a maximum longevity for this type of treatment.
For more information visit www.europe.gc.dental/en-ER/products/gaenialuniversalinjectable.
Authors
Professor Marleen Peumans (Belgium) graduated at the KUL (University of Leuven, Belgium) and is specialised in adhesive dentistry. Currently, she is head of the department of restorative dentistry of the same university.

Dr David Geštakovski (Croatia) graduated at University of Zagreb. After graduation he moved on short period of time to work in Dublin (Ireland). Nowadays he works in private dental office in Zagreb. He is member of Croatian Academy of Aesthetic Dental Medicine and European Society of Cosmetic Dentistry.

Dr Jacopo Mattiussi (Italy) graduated in Dentistry and Dental Prosthetics with honours at the University of Genoa. Currently, he is working in several dental practices in the conservative, prosthetic and endodontic field with a particular passion and attention for aesthetic and adhesive dentistry.

Dr Kostas Karagiannopoulos (United Kingdom) graduated at the Queen Mary University, whereafter he specialized in prosthodontics in King’s College (London, UK). Passionate about education and comprehensive dentistry, he is currently offering patient care in two specialist clinics near London and teaching training specialists at King’s College.

References:
- Terry, DA. Restoring with Flowables. Quintessenz Publishing. 1st Edition 2017.
- Terry DA, Powers JM. A predictable resin composite injection technique, Part I. Dent Today. 2014 Apr;33(4):96, 98-101.
- Terry DA, Powers JM, Mehta D, Babu V. A predictable resin composite injection technique, part 2. Dent Today. 2014 Aug;33(8):12.

