 In this month’s Dental Student’s Guide, Hannah Hook covers infective endocarditis, explaining what to look out for and treatments.
In this month’s Dental Student’s Guide, Hannah Hook covers infective endocarditis, explaining what to look out for and treatments.
Infective endocarditis (IE) is a rare but potentially life-threatening infection. Transient bacteraemia most commonly causes it.
The bacteria in the blood stream reach the heart. This leads to inflammation of the endocardium of the heart valves.
If infection is left untreated, bacteria are left to multiply and can lead to destruction of the heart valves and eventually heart failure.
Bacteria can also form emboli, which can dislodge and block small arteries in the brain. This can result in a stroke.
IE is difficult to diagnose but due to its severity improved outcome relies on prompt diagnosis and treatment.
Infective endocarditis
It was previously believed that the biggest risk factor for IE of oral origin was invasive dental procedures leading to high-grade bacteremias.
However, it is now believed that daily activities such as tooth brushing, flossing and chewing result in cumulative low-grade bacteremias. These play a more significant role in causing IE.
In the UK prior to 2008 antibiotic prophylaxis was recommended prior to invasive dental treatments to prevent IE in groups of patients at increased risk.
The most commonly prescribed drug for prophylaxis against IE was 3g Amoxicillin.
In 2008 NICE guidance changed to highlight that routine prophylaxis against infective endocarditis was no longer routinely recommended for dental procedures.
In 2016 the guidance amended further. It is therefore currently: ‘Antibiotic prophylaxis against infective endocarditis is not recommended routinely for people undergoing dental procedures’
Whilst the number of cases of IE originating from invasive dental procedures remains low, it is also important to be aware of the symptoms, risk factors and implications on dentistry.
Symptoms
- High temperature
- Chills
- Headache
- Joint and muscle pain.
Patients at increased risk
- Previous infective endocarditis
- Valve replacement
- Acquired heart disease with stenosis or regurgitation
- Structural congenital heart disease
- Hypertrophic cardiomyopathy – enlargement of cells of heart, thickening of walls of heart chamber.
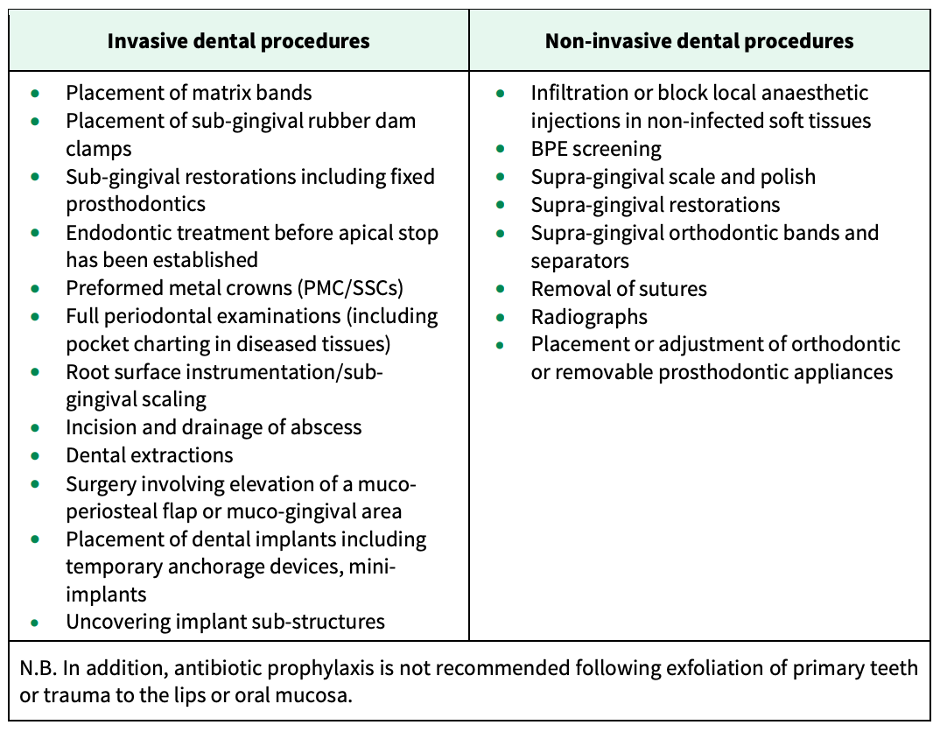
Invasive versus non-invasive dental procedures
Below is a table (Figure 1) produced by the SDCEP. It outlines which dental procedures are invasive or non-invasive.
Dental management
For the small number of patients that may require antibiotic prophylaxis there is currently no clear information available on which antibiotic prophylaxis to prescribe.
This is confusing for dental practitioners. It has also led to a wide variation in prescribing regimes.
The SDCEP has therefore created guidance on the management of patients at an increased risk of IE.
General information
- Make sure that patients at an increased risk of IE are aware of their risk
- Reiterate the importance of good oral health
- Explain the symptoms of IE
- Discuss the risks of invasive procedures
- Record the discussion in the patients notes
- Investigate and treat any episodes of dental infection promptly to reduce risk of IE developing.
Routine management
- Provide information about prevention, including the possible risks and benefits of antibiotic prophylaxis and explain why clinicians don’t routinely recommend antibiotic prophylaxis
- If the patient requests antibiotic prophylaxis discuss this further with their cardiologist to get advice.
Non-routine management
- Some patients at an increased risk of IE may fall into the non-routine management sub-group
- Assess patients and liaise with their cardiologist to determine the need for antibiotic prophylaxis for invasive dental procedures. If, following discussion, the patient doesn’t require antibiotic prophylaxis, they should return to the ‘routine management’ group
- If considering antibiotic prophylaxis, make sure to inform the patient about the potential risks and benefits associated.
Antibiotic prophylaxis suggestions
- Patients should give a prescription for the antibiotic prophylaxis prior to their invasive dental treatment
- They should take the antibiotic prophylaxis in practice 60 minutes before the planned procedure
- If a patient has received a course of antibiotics in the six weeks prior to the procedure, chose a different antibiotic class for prophylaxis
- If the patient is not allergic to penicillins the prophylaxis of choice is: Amoxicillin, 3g oral powder sachet
- And if the patient is allergic to penicillins the alternative is: Clindamycin, two x 300mg capsules (600mg total).
* Bear in mind that antibiotic prophylaxis doses are different for children.
Key points
- IE is a rare but life-threatening condition. It most commonly occurs as a result of transient bacteraemia
- Patients at an increased risk of IE are those with valve replacement, acquired heart disease, structural congenital heart disease, hypertrophic cardiomyopathy, or previous episode of infective endocarditis
- Patients at an increased risk of IE undergoing invasive dental procedures require special consideration as to whether they require antibiotic prophylaxis prior to treatment
- The most commonly prescribed antibiotic prophylaxis for IE prior to invasive dental procedures is Amoxicillin 3g and Clindamycin 600mg.
Catch up with previous student’s guides:
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

