 MDDUS dental adviser, Mike Williams, looks at barriers to best practice.
MDDUS dental adviser, Mike Williams, looks at barriers to best practice.
If you spend enough time in the company of dentists, sooner or later you will hear one say: ‘I can only do things one way.’
They are talking about the way they treat patients. There is usually an unsaid, but roundly acknowledged, addition, which is: ‘…That is the best way, obviously’. And a further unspoken comment: ‘…Not like one or two others I might care to mention.’
They mean it too. It is a genuine belief, which we all hold to an extent. We always try to do the best for our patients; we certainly never set out to cause them harm or distress. That is one of the reasons why we sometimes find it difficult to deal with complaints.
A corridor of acceptability
One might counter that: ‘I can only do things one way’ view by asking: Does that mean the treatment you provide for the first patient on a Monday morning, after a very enjoyable weekend away, when you perhaps ate a little too much, drank a little too much and didn’t get enough sleep?
Is it the same as the treatment you provide for the patient who can’t possibly lie flat in the chair, or who needs to rinse and spit every 30 seconds, or who smells and can’t keep their mouth open?
Would that include the treatment you offer a patient seen late on a Friday afternoon, when you’ve been running late since 9am, worked through lunch and you have to be finished promptly at 5pm to get to a personal appointment?
Is it the same as the treatment provided for your mother when all you have to do is a small filling and have booked out the entire afternoon to do it?
The truth is we don’t ‘only do things one way’.
We tend to provide treatment that lies within a corridor of acceptability. Most of the time we are right down the centre, and all is well. Our patients are happy and so are we.
From time to time we may stray toward one side or the other, but the treatment is still acceptable. Every now and then, we crash into the wall and the treatment has to be replaced, or the fee refunded or there may be a complaint.
Occasionally we end up dealing with solicitors and/or the regulator. Of course some clinicians’ corridors are wider, or narrower than others’.
(If you are enjoying and can relate to this article, please click the links to read parts two and three)
Life in a day

In the table I have listed a few circumstances that might contribute to either a good or a bad day. We may each have slightly different lists, but there are probably a number of common features that we see on any clinician’s list.
So what do you think contributes to a good or bad day?
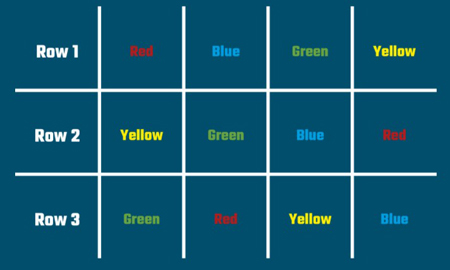
Let’s try a thought experiment. Take a look at the first image, and in your mind, state the colours as fast as you can.

Now look at the second image. Again in your mind, state the colours as fast as you can.
Now look at the third image. Again, in your mind, state the colours as fast as you can. Remember state the colour you see, not the word you can read.
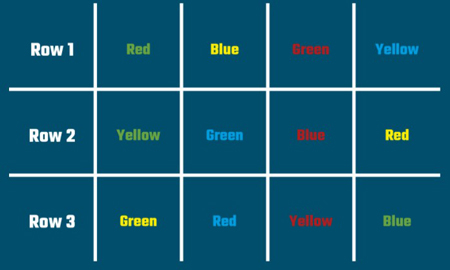
Many people find this a little more difficult, and it takes a little longer.
Stroop test
This is called a Stroop test – named after the American cognitive psychologist J Ridley Stroop. It is designed to demonstrate how we process relevant and irrelevant information. More straightforwardly it demonstrates that performing even a simple task in unfavourable or ‘incongruent’ circumstances is difficult.
So, suppose all you have to do is carry out a small routine restoration, bring the patient in, make sure you have the right patient, check the medical history, check the treatment plan and consent, make the patient numb and do the filling.
But…you are running late.
You are working with an agency nurse who has worked in the practice for two days and doesn’t yet know where everything is kept. And you cannot find the radiograph and the suction is playing up again. The patient is irritated because you kept them waiting and they can’t lie too far back, and you know you have to be out of the practice by a certain time, because you have an appointment of your own.
Will you work more or less effectively given these added factors?
Take a minute…or two
It is not possible to eliminate all interruptions and irritations. But it is a good idea to try to minimise and control them where possible.
Plan ahead, set rules about interruptions, use checklists and team briefings.
At the very least, when these irritations and interruptions become apparent, it is important to recognise that they can impact on the treatment. They can impact on that ideal, centre-of-the-corridor, ‘I can only do things one way’ treatment. This is when we lose concentration, cut corners cut, make mistakes, treatment goes wrong and we get complaints and claims.
Take a step back, take an extra minute or so. Maybe even decide to reschedule what you were going to do. These are decisions under your control.
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

