





If you’re ready for a confidential discussion with Practice Plan about the next steps in converting to private dentistry, leave your details below.










An example of a longer piece of text over a paralax scroller background to show a range of movement as the user scrolls past.
An example of a longer piece of text over a paralax scroller background to show a range of movement as the user scrolls past.
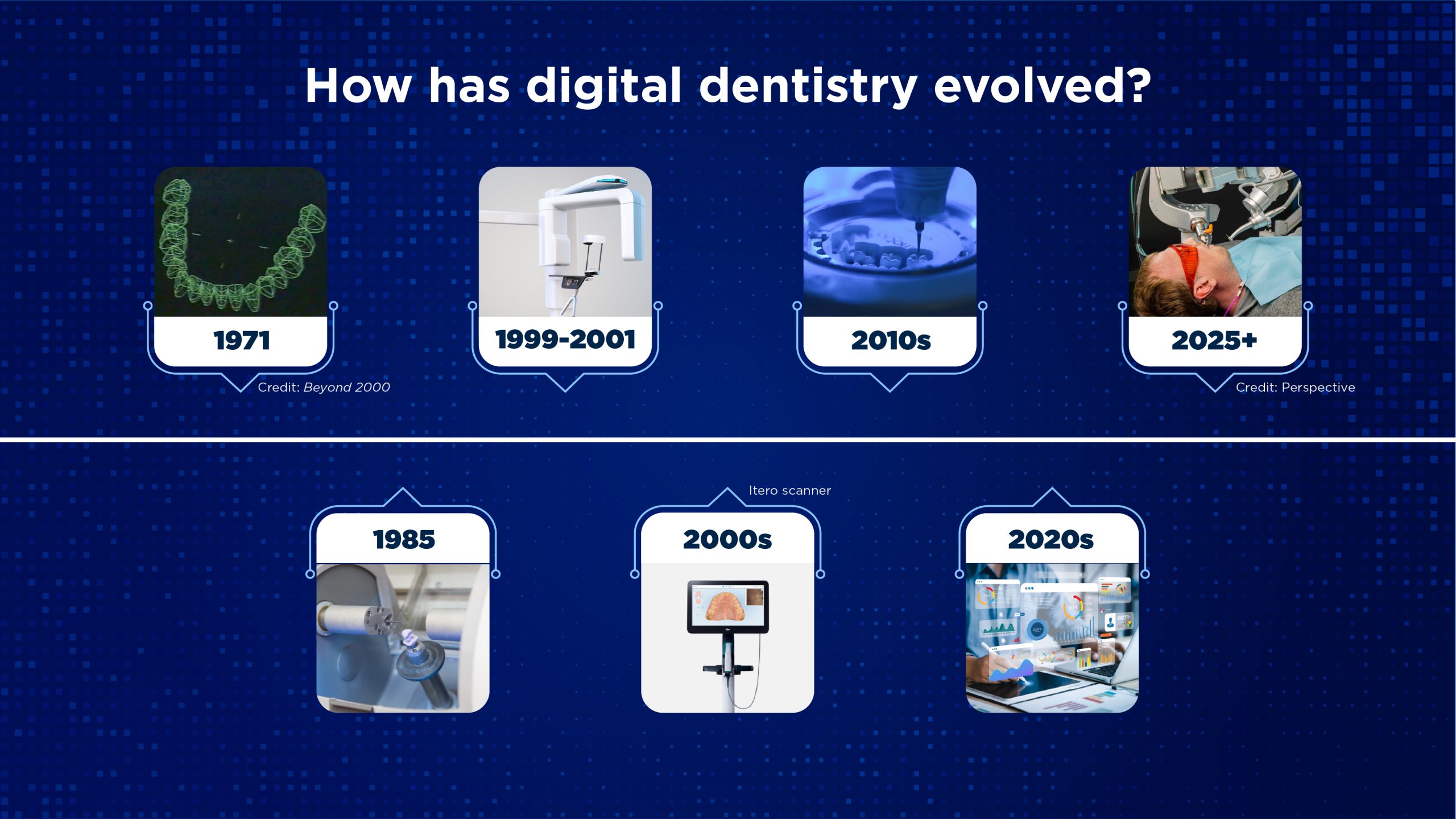
The roots of digital dentistry can be traced back to the mid-to-late 1980s, when pioneering CAD/CAM systems such as CEREC were introduced to enable chairside design and milling of ceramic restorations. These early systems were groundbreaking but far from perfect – they were expensive, had steep learning curves, and offered results that were often inferior to those from skilled technicians. As a result, adoption was initially limited to a small number of technology-forward practices.
Simultaneously, digital radiography began to emerge, offering dentists faster imaging, the ability to manipulate contrast and magnification, and reduced radiation doses for patients. In its early phase, digital radiography was largely confined to well-funded practices, but over time it became standard.
The pace of innovation accelerated in the late 1990s and early 2000s with the development of more user-friendly and accurate intraoral scanners. These devices replaced traditional impression materials in many cases, improving patient comfort and clinical precision. By the mid-2000s, cone beam computed tomography (CBCT) brought 3D imaging into the general practice, transforming treatment planning in implantology, endodontics, orthodontics, and even oral surgery.

This Dentist was Sad whilst working in the NHS
Julian Caplan is a leading voice in digital dentistry and the inaugural president of the Digital Dentistry Society UK. Here, he explores the early challenges of digital adoption and how the experience of use has transformed over the past 30 years.
Francois Duret developed the first intraoral scanner in 1971. He linked this technology with a milling machine to allow for in-surgery porcelain restorations to be produced.
As with all new ideas, there are well known stages of development ranging from innovators and early adopters through to laggards. In order for new ideas to become mainstream a so-called ‘chasm’, as described by Geoffrey Moore, needs to be crossed from these early adopters in order for these technologies to become common usage.
We are now at the stage where, with scanners that are more affordable and considerably easier to use than the first intraoral scanners, this chasm has truly been leapt.
In order for dentists to feel comfortable in utilising this technology, an important advancement is the considerable improvement in the precision of intraoral scanners. Along with vastly improved speed of scanning, this has given dentists the confidence to provide either highend immediate restorations for their patients or to apply this technology to many other dental techniques and clinical situations.
Some examples of these are:
- Assessing occlusion to diagnose pathological interferences
- Greatly simplifying the production of occlusal splints
- Monitoring changes in occlusion and morphological changes
- The production of dental prostheses by either milling or printing from the digital data gained
- Combining it with other technologies such as dental printing to produce multiple restorations in a more timely manner, CBCT scans to allow for more accurate implant planning, and the production of surgical guides for the placement of dental implants.
Now he’s happy after the transition to Private Dentistry
There are many benefits to moving your practice into the realm of digital. These include:
- Greater patient comfort, especially with the scanner heads becoming smaller and the scanning speed vastly increasing
- The ability to assess preparation design and clarity to allow immediate feedback for refinement prior to the final definitive scan, rather than waiting for feedback from the technician that may require the patient to return for a second visit
- Immediate adjustment of part of a scan rather than the old issue of having to retake impressions due to air bubbles, drags and other distortions
- More streamlined and controllable workflows for many procedures
- Improved communication with dental laboratories with immediate dental technician feedback.
How is the technology being used?
There are three main technologies that are used in intraoral scanning:
- Triangulation
- Confocal microscopy
- Active wavefront sampling.
The assessment of the scanning accuracy of this technology is usually done locally (single tooth) or globally (across the arch). A study by Osnes and colleagues (2021) showed that the arch width between the second maxillary molars was 55.44 mm with a laboratory standard Solutionix scanner, while a scanner using confocal microscopy measured it at 55.439 (+/- 0.075)mm.
In comparison, a scanner using triangulation measured the same distance to be 54.672(+/- 0.65)mm. The mean proportion of the confocal microscopy scans deviating beyond 0.1mm when compared to the Solutionix was 0.7(+/-2.0)%, whereas the equivalent for the triangulation scan was 42.1(+/-2.5)%.
This highlights the difference in accuracy depending on the technology used.
Digital dentistry has come a long way since its inception in 1971. The multiple technologies, ranging from intraoral and CBCT scanners to printers and upcoming AI advancements, are and will make a profound change in the lives of dentists, as well as the treatment and experience their patients receive.