This month, Hannah Hook explores Le Fort fractures, including classifying each one and the best treatment option for the patient.
In 1901 French surgeon Rene LeFort published a classification of midface fractures. It was based on his studies conducted on cadavers.
He assessed predictable patterns of fracture of the midface and ultimately described three lines of weakness.
As a result, this is known as the Le Fort classification and is divided into Le Fort I, Le Fort II or Le Fort III. Each are them are determined by the levels of the transverse fractures (Figure 1).
Le Fort fractures result in a separation of the maxilla from the rest of the skull. Consequently, they may also cause a dental malocclusion.
In addition, Le Fort injuries are not overly common but do occur, usually as a result of severe blunt force trauma to the face.
Le Fort I
- Horizontal fracture
- Fracture line runs through the maxilla and the pterygoid plates at the level of the nasal floor
- Results in separation of the hard palate from the maxilla.
Le Fort II
- Pyramidal fracture
- Extends from the anterior portion of the medial orbital walls, orbital floor, inferior orbital rims to the posterior maxilla and pterygoid plates.
Le Fort III
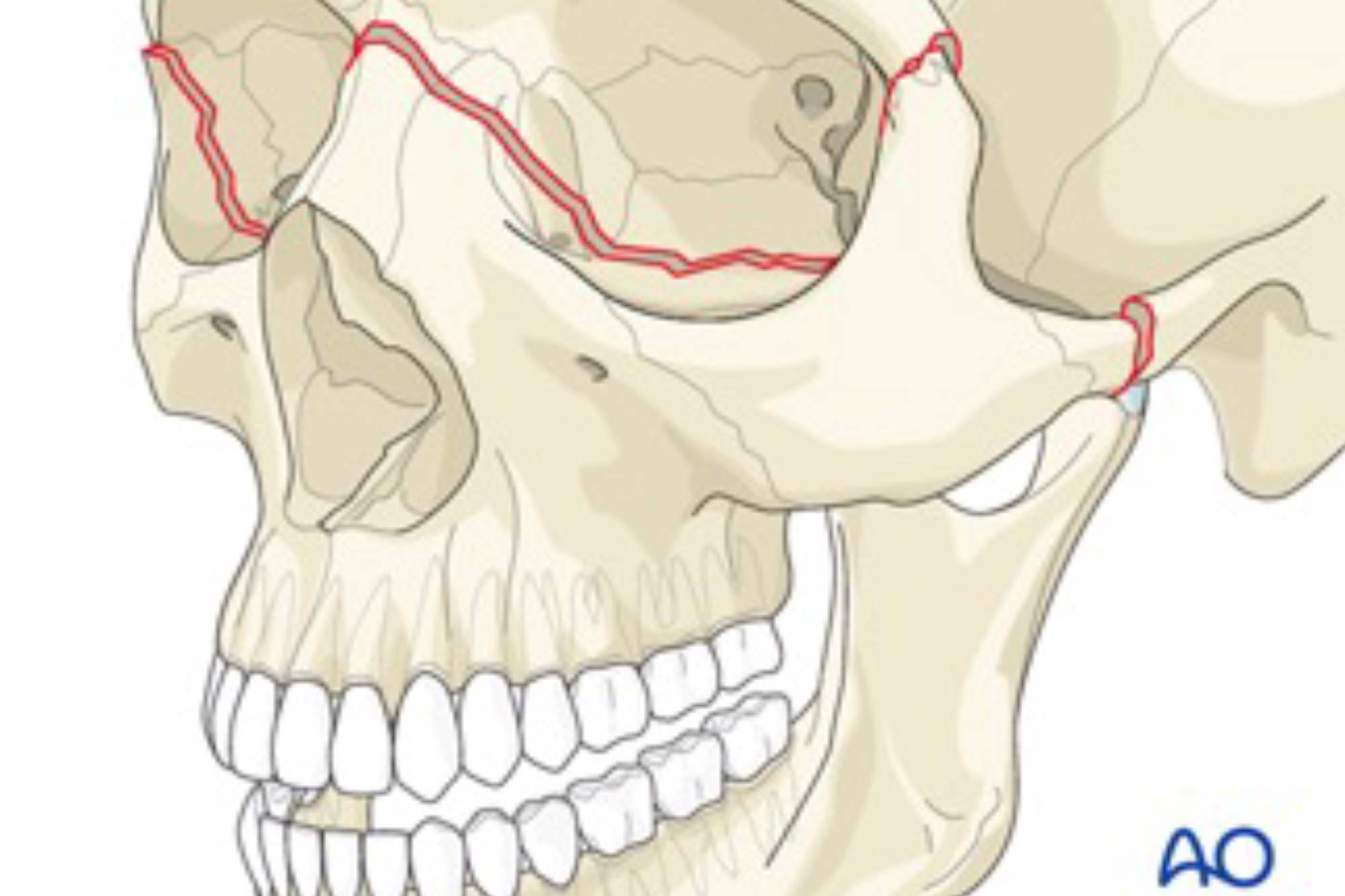
- Separation of the maxilla from the base of the skull
- Fracture extends through the nasofrontal suture, medial and lateral orbital walls, zygomaticofrontal suture, zygomatic arch and pterygoid plates
Assessment
- ABCDE approach
- Make sure the airway is patent and not compromised. If it is compromised, the patient may require intubation
- The patient should be assessed by an emergency department clinician to clear them of a head injury
- Look for any obvious facial asymmetry
- Palpate the face for any area of acute bony tenderness or bony steps
- Assess sensation by checking the branches of the trigeminal nerve
- Check for any signs of reduced mouth opening
- Assess the eyes, check visual acuity, restriction of eye movement, diplopia, reactivity of pupils to light
- Intraorally assess the patient’s occlusion and any dental trauma
- Check for mobility of the maxilla.
Investigations
A CT scan of the head should be completed to allow visualisation of the facial fractures.
Treatment
The three methods of treatment of a Le Fort fracture are conservative management, closed reduction or open reduction internal fixation.
In addition, the type of treatment offered is highly dependent on whether the fractures are displaced and whether there is a malocclusion.
Conservative management
Indications:
- Non-displaced fractures
- Stable occlusion
- Edentulous patients with minimal fracture displacement
- Any factors preventing surgical intervention.
Also the fractures are left to heal without intervention.
As a result, patients are required to follow a very soft diet, take pain relief and avoid contact sports for approximately six weeks.
Closed reduction
Indications:
- Minimally displaced fractures
- Minor malocclusion
- Maxilla not overly mobile following repositioning.
Usually, closed reduction entails the use of intermaxillary fixation to hold the jaws in the correct position. This is to allow for stabilisation and healing.
As a result, patients are required to follow a very soft diet, take pain relief and avoid contact sports for approximately six weeks.
Open reduction internal fixation (ORIF)
Displaced fractures will likely require surgical intervention. This is usually done by open reduction and internal fixation (ORIF).
ORIF is where an incision is made and the fracture lines are exposed. The bones are repositioned to reduce the fracture lines.
In addition, metal plates are then placed across the fracture lines and screwed into the bone on either side. This will hold the bones in the desired position and stabilise the fracture.
As a result, patients are required to follow a very soft diet, take pain relief and avoid contact sports for approximately six weeks.
Key points
- Le Fort classification is a categorisation system for midface fractures, it includes Le Fort I, II and III
- The fractures are uncommon and usually occur as a result of great blunt force trauma to the face
- A thorough assessment and a CT head is carried out on a patient with a suspected Le Fort fracture
- The three main forms of treatment for Le Fort fractures are conservative management, closed reduction or open reduction internal fixation
- The best treatment option for the patient will depend on the severity of displacement of the fractures and whether there is a malocclusion present.
Email [email protected] for references.
Catch up with Hannah’s previous dental student guides
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

