 In the latest Prosthodontips column, we are presented with a case that has been treated using composite injection moulding (IM).
In the latest Prosthodontips column, we are presented with a case that has been treated using composite injection moulding (IM).
Composite resins have been around for a long time now and we have seen them grow in application, especially in restorative dentistry. Over the past fifty years, there has been development of adhesive technologies. As a result, the chemistry of our clinical practice is continually evolving.
These advancements have led to the latest generation of resin materials: heavily-filled injectable composite resins. Not be mistaken for flowable resins, injectable materials display similar viscosity to flowable materials during extrusion. Once applied, however, injectables tend to exhibit far less flow than their counterparts.
This thixotropic nature allows them to be used in a wide range of applications. Of these, however, the most interesting is the use of composite injection moulding (IM) in cases requiring aesthetic and/or functional rehabilitation.
Injection moulding is the technique of using a silicone stent to guide the external form of the definitive composite resin restoration. It is important to note that it is fully guided technique and hence is not reliant on advanced operative skills to produce predictable outcomes.
As the silicone stent is a direct negative of the diagnostic wax up, the exact reproduction of the anatomical details and textures in the wax up is easily achieved intraorally. To demonstrate this, I will present a case that has been treated using this technique.
Injection moulding in practice
The patient presented is a 28-year-old male with severe generalised erosive toothwear. His presenting complaint was the general poor appearance of this teeth, which he attributed to the colour, staining and also irregularity of the maxillary incisal edges.
As the maxillary and mandibular teeth are still in occlusal contact, we know the toothwear has resulted in dentoalveolar compensation. So following a consultation period, the patient agreed to proceed with care using composite resin restorations. A full mouth rehabilitation was planned (figures 1, 2 and 3)



Records were taken to allow mounting of study models in centric relation. The records included alginate impressions, occlusal records and also a facebow record. The occlusal records shown were take to record the mandible in centric relation. A Lucia jig was used to locate this position and, additionally, an occlusal registration made using a silicone material. The models were subsequently mounted by a commercial laboratory.
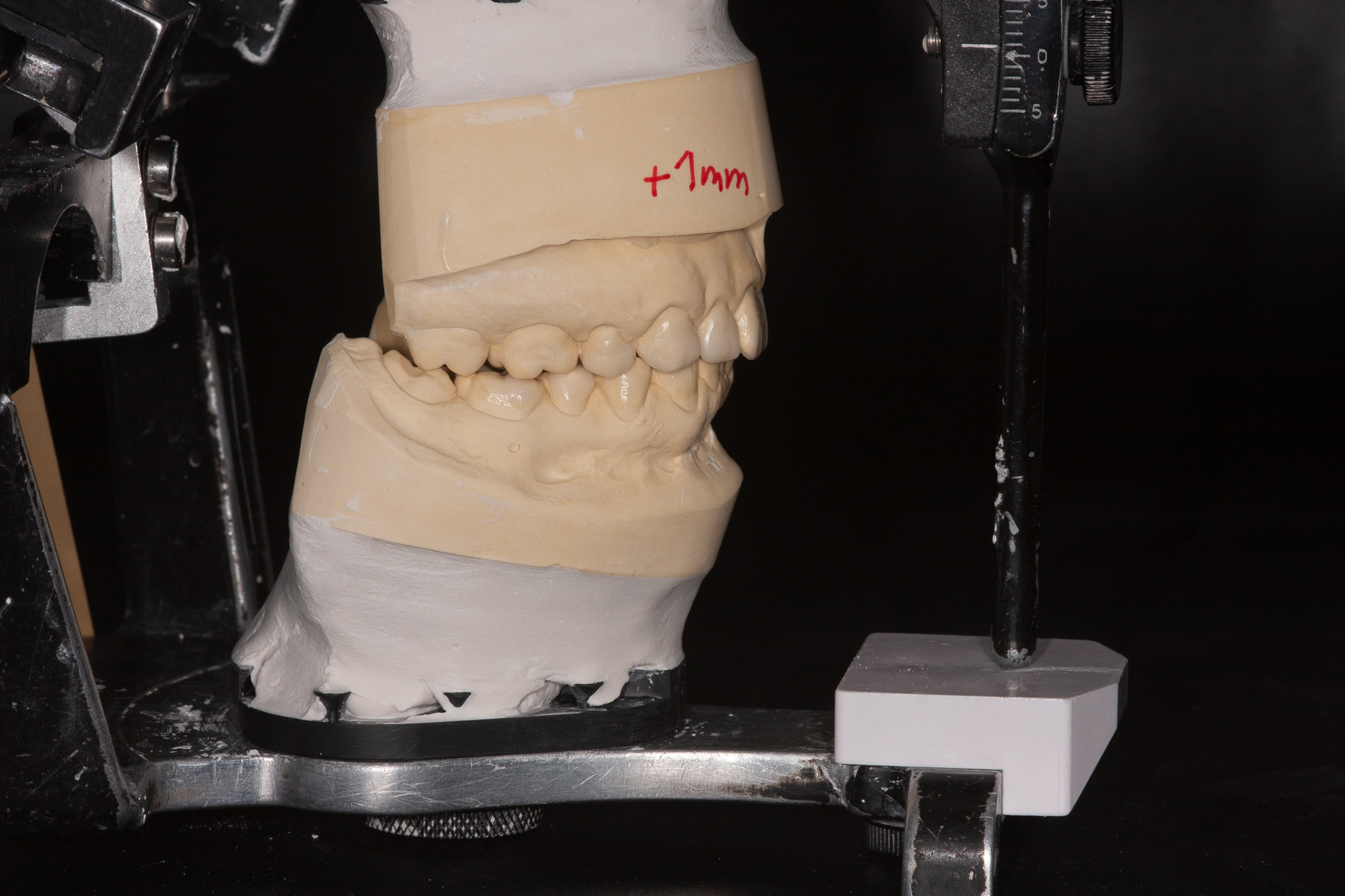
A full mouth diagnostic wax up at increased occlusal vertical dimension was completed. It was necessary to increase OVD by 1mm beyond the retruded contact position to allow sufficient bulk of restorative material (figures 4 and 5).

An intra-oral mock was completed using a bisacryl material. The material was extruded into a putty matrix of the wax up and the matrix seated intraorally. Once the material was set, the matrix was removed to allow assessment of the aesthetic and functional elements of the mock up (figure 6)

Restored
Firstly, the maxillary arch in its entirety was treated. A putty matrix was used to visualise space for the composite resin. Minor preparation was carried out where necessary once existing restorations were removed. In addition, the arch was treated on an alternate tooth basis.
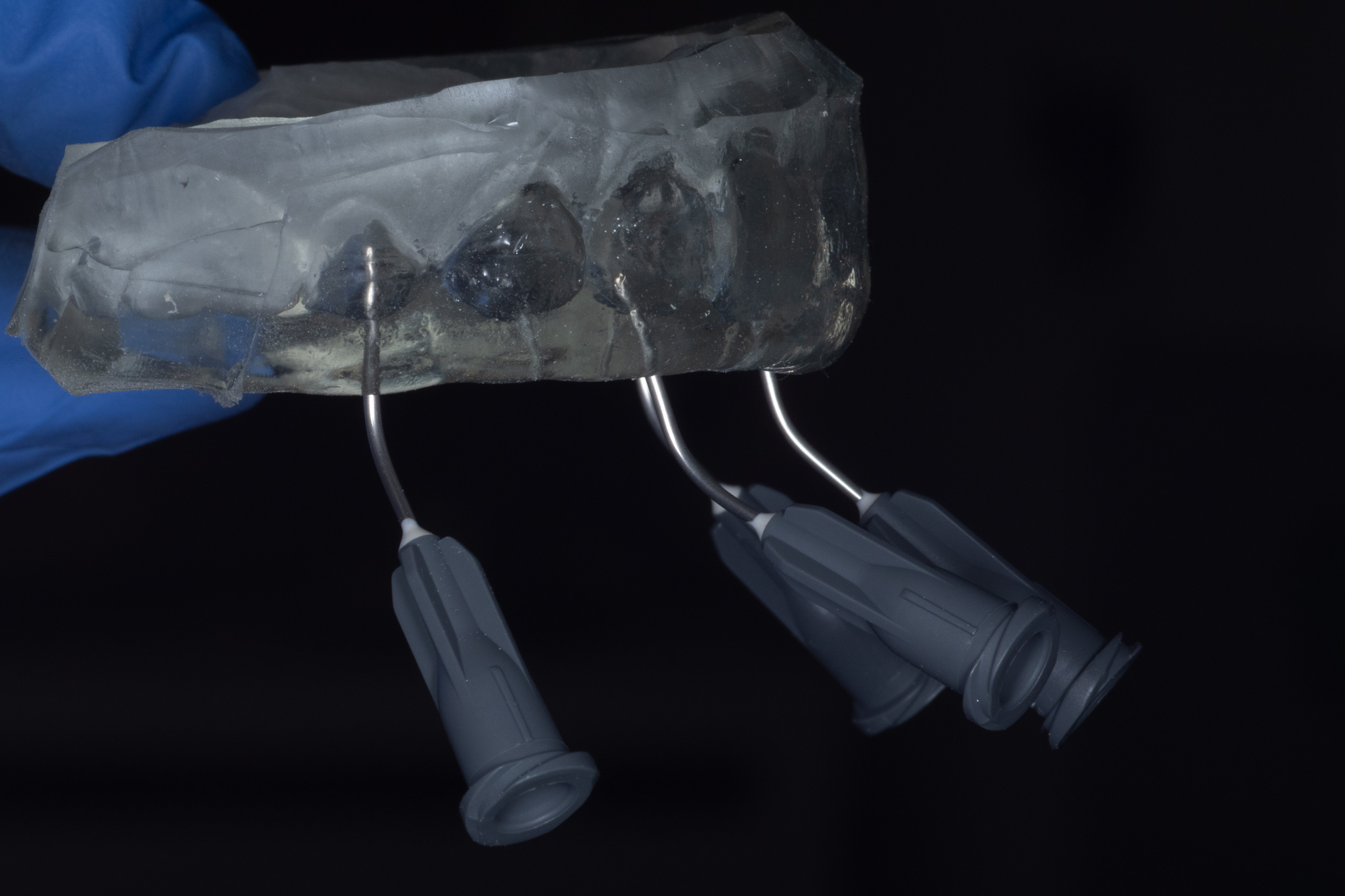
Following the placement of retraction chord, the teeth were isolated with PTFE tape. Next, the teeth were air abraded and also prepared for bonding using a three-step protocol. The clear silicone stent was then used to restore every alternate tooth. The remaining teeth were subsequently restored in the same manner (figures 7, 8, 9, 10 and 11).




Following restoration of the mandibular restoration, the occlusal was checked and some minor adjustments were carried out. A simple polishing procedure using interproximal strips and a two-step silicone brush protocol was used. The patient was extremely happy with the final aesthetic outcome. They also report no functional problems.
The source of erosion has been identified and dietary modification also implemented. In addition, the restorations will be protected through the nightly use of an occlusal splint (figures 12, 13, 14 and 15).




Previous Prosthodontips:
- The value of ceramic abutments
- Occlusion revisited: part two
- Preparing for excellence: how to produce an excellent crown preparation
- Occlusion revisited: part one
- Smile design
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

