Tom Witcher, a specialist orthodontist at Total Orthodontics Haywards Heath, part of Bupa Dental Care, shares his method for deciding whether to extract poor prognosis first molars in mixed dentition.
A significant number of early referrals to specialist orthodontists concern the poor prognosis of first molars and the timing of their extraction.
In our practice, approximately 10% of early referrals under the age of 10 are primarily or only concerned with poor prognosis first molars.
First molars are frequently compromised at a young age through caries or molar-incisor hypomineralisation (MIH).
The sensible questions of if and when they should be extracted regularly arise before the patient is dentally ready for definitive orthodontic treatment.
After clinical and radiographic examination and discussion with the GDP in borderline cases, if extractions are indicated, I tend to group these patients into one of three categories:
- Extract now for the best outcome via spontaneous space closure
- Delay extractions until later to use the space for definitive orthodontic treatment
- Extract now and accept future orthodontic problems.
1. Extract now for the best outcome via spontaneous space closure
In this group, we remove the first molars and await an almost like-for-like replacement by the second molars. They migrate mesially to erupt where the first molars would have been.
This can be a really elegant way of dealing with the first molars of a hopeless prognosis.
The typical patient in this group would be about age eight to 10 and have close to a class I occlusion with minimal crowding. This is essentially any patient where future extraction-based treatment will be unlikely.
The stage of dental development is, however, more important than chronological age.
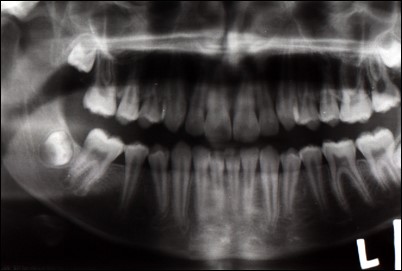
The OPG would ideally show that the second molar root bifurcations are starting to calcify for the best chance of spontaneous space closure – too early and the second premolars can drift distally; too late and the second molars tip mesially, leaving residual space and/or poor contact.
Having third molars present on the OPG would lend weight to extracting the first molars because this likely means the patient will ultimately have two erupted molars.
A positive side effect will be to relieve future crowding in the third molar region. In some patients, this might reduce the chances of a trickier and riskier third molar extraction at a later date.
These images of two OPGs of the same patient demonstrate the migration of the right second molars after losing the right first molars. The angle of the LR7 is not perfect, but it is a relatively easy job to upright as part of any orthodontic treatment.

2. Delay extractions until later for definitive orthodontic treatment
If a patient has a malocclusion likely to require future extractions to help their orthodontic treatment in the permanent dentition, then trying to keep the first molar in situ is often worthwhile.
These might be cases where significant crowding or an increased overjet is present in the permanent dentition.
The first molar would need to be temporised normally until the permanent dentition have erupted. This includes the second molars to allow anchorage reinforcement.
This would require a cooperative patient and a tooth with at least hope of lasting a few trouble-free years if temporised.
3. Extract now and accept that there may be more complex treatment required later
Essentially, these are the patients in group two where temporisation of the first molars is not possible. This is perhaps because of poor cooperation, but sometimes because the tooth is just too far gone.
From a pain management and dental health perspective, extracting the first molars outweighs the benefits of attempting to maintain them.
They may ultimately require further extractions, usually premolars, in the permanent dentition to allow their malocclusion to be treated.
Balancing and compensating extractions
These would be assessed on a case-by-case basis. But three general rules are:
- Balancing extractions (removing the contralateral tooth in the same arch) are not required for first molar extractions
- Compensating extractions (removing the opposing upper first molar) are routinely carried out for lower first molar extractions to prevent overeruption. This will also allow the development of a normal molar relationship.
Compensating extractions of healthy lower first molars for lone upper first molar extractions are not indicated.
Read previous Total Orthodontics columns:
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

