Raman Aulakh explains the power of biomechanics in a force-driven approach to clear aligner therapy and presents a case study.
Understanding the power of biomechanics in aligner therapy
One of the most valuable lessons I’ve learned in clinical practice is the importance of applying biomechanics to aligner therapy. It’s the difference between passively nudging teeth into place and actively guiding them with precision toward a planned outcome.
This becomes especially critical in complex cases, where transitioning from a mindset of displacement-driven mechanics to force-driven biomechanics is essential.
Steering versus pushing: the force-driven aligner system
A useful analogy for understanding force-driven systems is the difference between pushing a shopping trolley and steering a car. Pushing the trolley involves effort and guesswork – it often doesn’t go where you want.
Steering a car, on the other hand, offers controlled, predictable movement. Displacement-driven mechanics follow the trolley model, relying on the aligner’s shape to push teeth into position. While this works for simpler movements like tipping, it frequently falls short for more complex movements such as torque, bodily translation, or extrusion.
Force-driven systems resemble the car’s steering system – applying targeted, intentional forces to direct tooth movement. This approach includes torque programming, optimised attachments, pressure points and integrated torsion within the aligner material to generate the required moment of force for root control.
Align seeks to achieve this through three innovations: SmartForce directs force precisely using attachment design, pressure points, and built-in torsion. SmartTrack, a flexible and durable material, aims to deliver a more consistent force. SmartStaging sequences staging shifts strategically for anchorage control and consistent force systems. But beyond the marketing language, what does this actually mean for us as clinicians?
Why force-driven mechanics are essential
Even with the most advanced aligner materials, plastic behaves like plastic – it bends, flexes and deforms. The challenge lies in these inherent material property limitations, particularly for complex movements.
However, with a thorough understanding of biomechanics and utilising the force-driven system, we can overcome these challenges. As clinicians we have the control of applying additional torque, using auxiliaries like elastics, attachments, modifying staging, and often overcorrecting movements to compensate for expected lag.
Evidence and predictability of torque and root movement
From both experience and evidence, torque and root movement remain among the least predictable outcomes in aligner therapy. Early papers such as Rossini and colleagues (2015) found aligners were ineffective in achieving significant torque changes, while Simon and colleagues (2014) showed only ~42% of planned incisor torque was expressed clinically. Haouili and colleagues (2020) reported a mean accuracy of ~50% across all movements, with complex ones like root translation often underperforming.
More recently, Castroflorio and colleagues (2023) reaffirmed the challenge of achieving root control without compensatory strategies. To overcome this, I rely on overcorrection for specific movements, torque staging to avoid uncontrolled tipping, attachment planning to give priority to certain movements and controlled force application through staging. All of which are discussed in more recent literature and finite element studies as methods to be considered to increase predictability.
Case study: creating space for a missing UL3 with force-driven mechanics and Invisalign
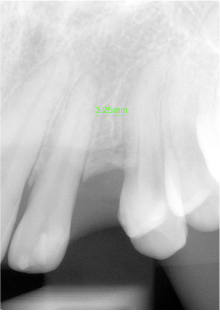
A recent case in my clinic involved creating space for a missing upper left canine (UL3). Initially, there was only 4.3mm of space at the crown level and 2.5mm between roots – insufficient for implant placement. Our goal was to achieve bodily movement and parallel root alignment and adequate space for the implant.
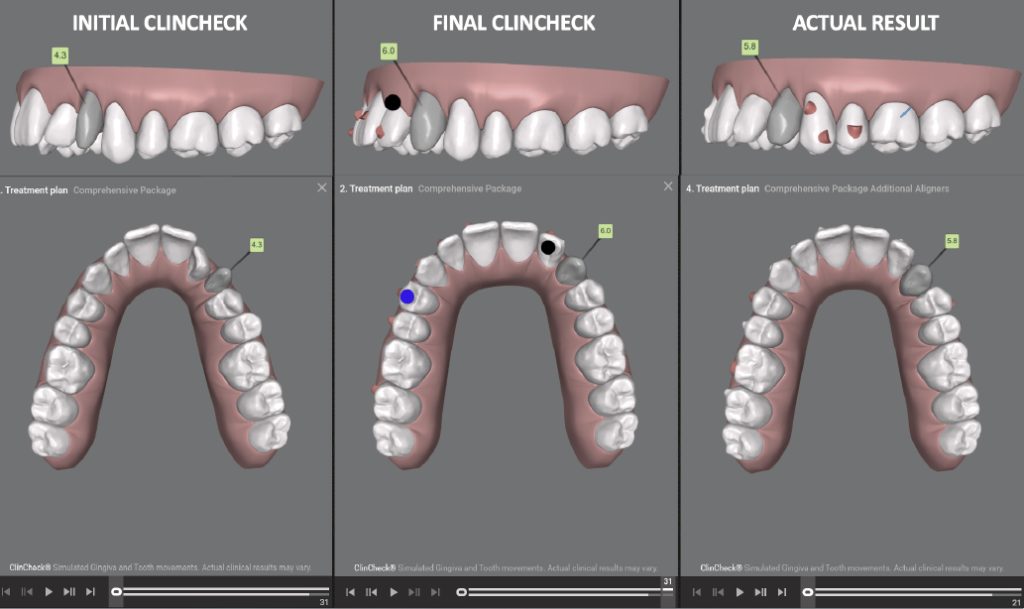
Initial set of aligners:
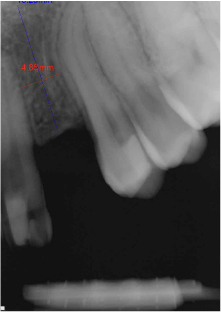
We started without over-engineering the plan and aiming for 6mm of crown-level space. While this achieved 5.8mm coronally, the roots remained only 3.8mm apart, creating a triangular space – a clear indication of uncontrolled tipping and the limitations of predictability with root movements.
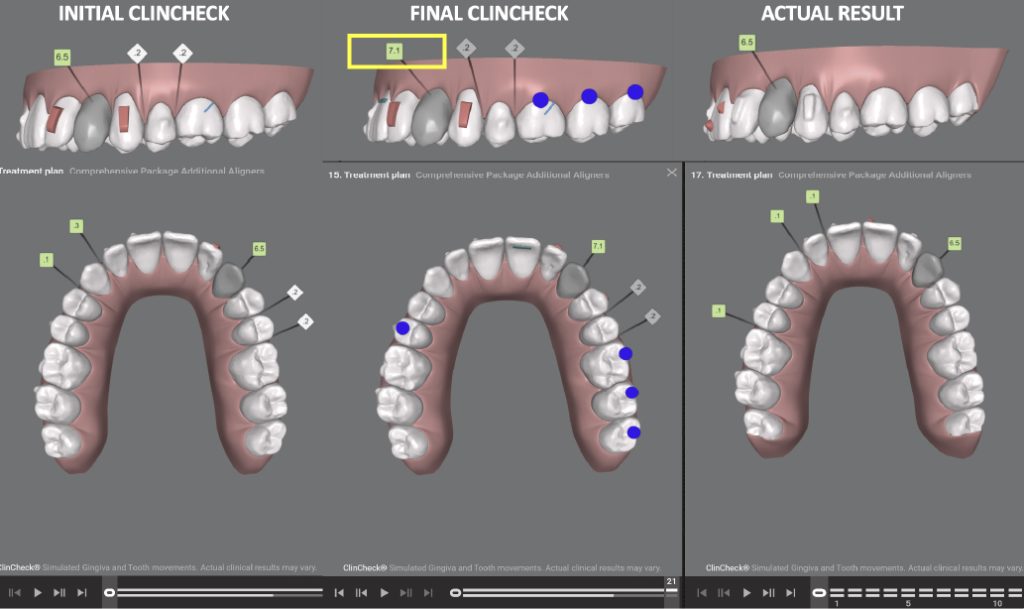
Additional aligners:
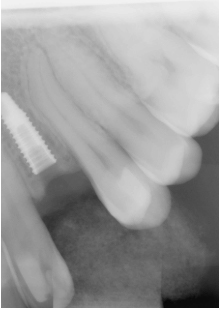
In the final refinement phase, we employed a force-driven strategy:
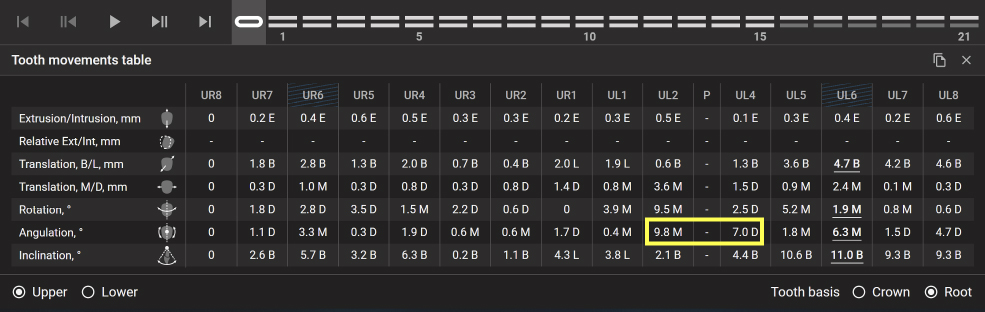
- Mesial root torque UL2 over-corrected by 7.5º to 9.8°
- Distal root torque on UL4 over-corrected by 5.0º to 7.0°
- Overcorrected space at crown level to 7.1mm to generate force to the plastic and attachments
- IPR between UL4–UL5 and distal to UL5 to facilitate distalisation.
This plan successfully created 6.5mm of space at the crown and 5.5mm between roots, verified radiographically. The roots were parallel, enabling appropriate space for implant placement. In effect, controlled force application transformed a tipping movement into root movement.

The fixed appliance analogy
This scenario closely parallels traditional fixed appliance techniques: using a push coil and gable bend on a rectangular arch wire to achieve bodily or root tooth movements. In aligner therapy, we replicate this through programmed torque, overcorrection, and rectangular vertical attachments in this case – all digitally planned, yet grounded in the same fundamental biomechanical principles.
Conclusion: Understanding predictability through biomechanics
Success in clear aligner therapy depends on understanding and applying biomechanical forces. In complex cases, relying on software staging alone is not sufficient. It’s the deliberate over-engineering and use of force-driven mechanics that elevates treatment outcomes from basic to advanced.
To determine the degree of overcorrection required, you must analyse the predictability of movements achieved in prior aligner stages, while also considering current evidence-based insights on predictability. Rigidly adhering to ‘set’ protocols, as sometimes promoted in training courses, can risk clouding clinical reasoning and hinder a tailored, patient-specific approach.
I encourage colleagues doing complex cases to embrace biomechanics in aligner therapy. Through advanced training such as the SAFE Clear Aligner Diploma you can develop the expertise to plan, predict and execute more challenging treatments confidently. We offer a pathway for both dentists and orthodontists. With this knowledge, you’re not just along for the ride – you’re in the driver’s seat, directing every case with increased precision and purpose.
For more information, visit alignerdentalacademy.com/clear-aligner-therapy-diploma/ or email [email protected].
This article is sponsored by the Aligner Dental Academy.
References:
- Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL (2015). Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod, 85(5): 881–889. doi:10.2319/061614-436.1
- Simon M, Keilig L, Schwarze J, Jung BA, Bourauel C (2014). Treatment outcome and efficacy of an aligner technique – regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health, 14:68. doi:10.1186/1472-6831-14-68
- Haouili N, Kravitz ND. Vaid NR, Ferguson DJ, Makki L (2020). Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop, 158(3): 420–425. doi:10.1016/j.ajodo.2019.12.015
- Castroflorio T, Sedran A, Trovati F, et al (2023). Predictability of orthodontic tooth movement with aligners: effect of treatment design. Prog Orthod, 24(1):47. doi:10.1186/s40510-022-00434-5

