 Mel Bastani explores the use of Botox to help treat TMD issues, as well as outlining how to assess the patients before treatment.*
Mel Bastani explores the use of Botox to help treat TMD issues, as well as outlining how to assess the patients before treatment.*
Facial aesthetics is a fantastic tool to use for preserving and enhancing natural features. But it can also be utilised for clinical problems too.
It’s shocking to understand that one in 10 people in the UK suffer with temporal mandibular dysfunction (TMD).
This condition has various different causes. So it is pivotal that you take a full detailed medical and social history of the patient before assessing the physical problem.
Treating TMD
One of the most popular reasons for Botox is for the treatment of TMD.
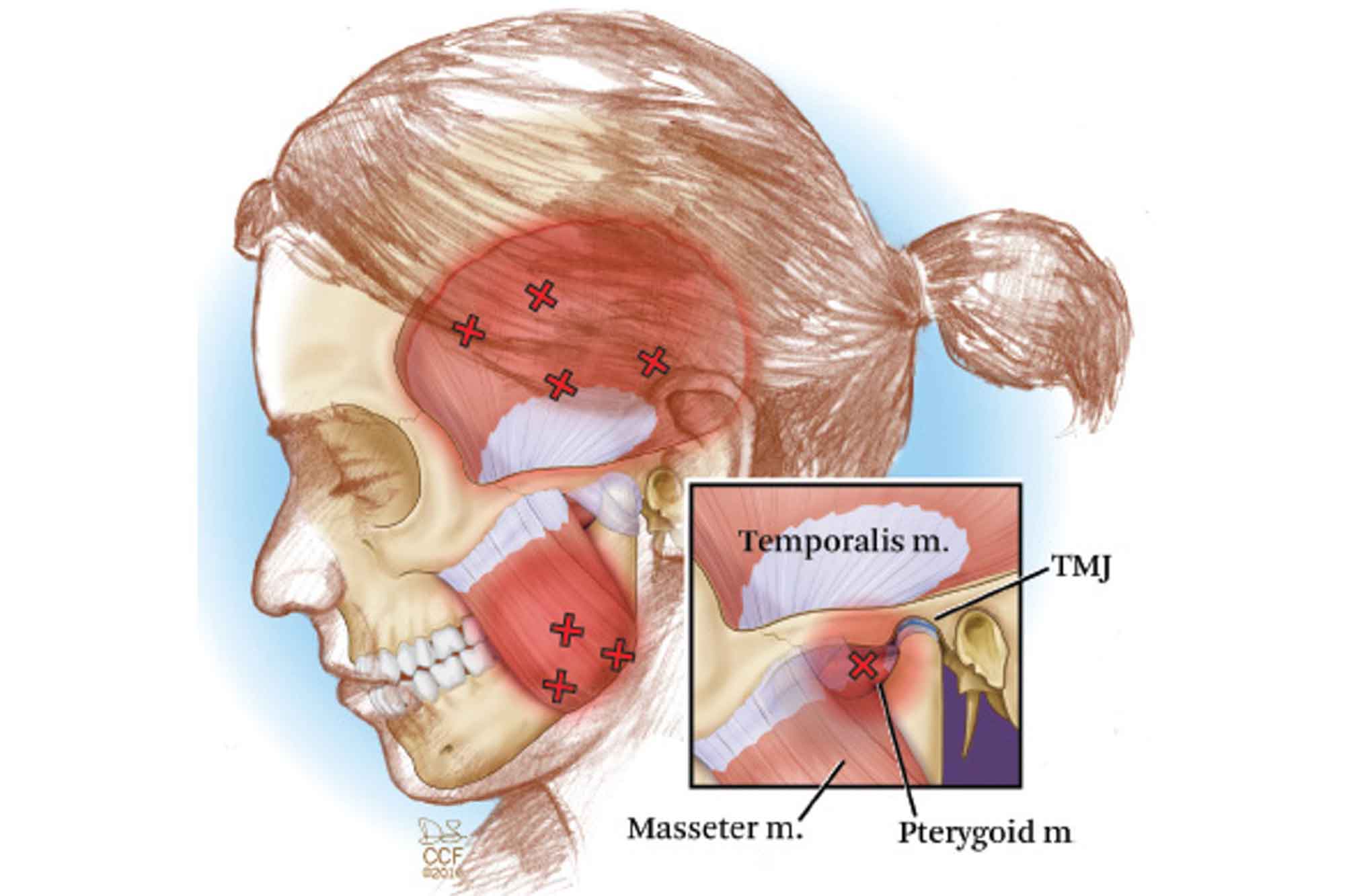
The TMJ is the two joints that connect your lower jaw to your skull. More specifically, they are the joints that slide and rotate in front of each ear, and consist of the mandible (the lower jaw) and the temporal bone (the side and base of the skull).
Some patients suffer with pain and stiffness around the jaw, ear and temple. This is usually caused by excess stress or over exertion of these areas through grinding or clenching.
As you can see in Figure 1, through clenching and grinding, these are the most common areas that are affected (marked with X).
When administering Botox, for example, in the muscle of mastication, it is vital to do an in-depth initial consultation and assessment. Injection in the wrong area or injecting too much in one muscle can lead to parafunction and can cause other problems later down the line.
If you’ve have already been trained in TMJ Botox treatment, you should be able to follow a few easy steps to help come to a conclusion during your assessment phase:
- Look out for clicking or bulging of the temporalis or masseter when the patient is clenching. When feeling the TMJ for these characteristics, you should also take into consideration if there is any deviation of the jaw when opening and closing. This would give an indication into whether or not parafunction is already present
- Use a ruler to measure the opening of the patient’s mouth. Usually non-suffering patients will have an opening of 4-4.5cm. Patients who suffer with TMD or clenching would usually have an opening of 3.5cm or less depending on the severity of the condition.
In a lot of cases the temporalis and masseter are the dominant muscles during clenching and mastication.
However, the lateral and medial pterygoids can sometimes become involved as the case of TMD becomes more severe.
Treatment
Ensure that when injecting muscles of mastication that the needle is aiming away from the front of the face.
Especially when injecting the masseter, you want to be careful that you do not inject the buccinator muscle. This may result in temporary paralysis and ultimately will lead to the patient having difficulties in chewing/mastication. The impaired functioning of this muscle can lead to repeated lacerations of the cheek mucosa.
Review
As with any aesthetic treatment, it is important to bring the patient in for a review.
Usually Botox can take seven to 10 days to fully take effect. So bring the patient in two to three weeks after treatment. Then review the outcome of treatment and assess patient satisfaction.
This will ensure that you have not affected surrounding areas around the treatment area and also assess whether the treatment has been successful in helping the opening of the mouth and therefore any pain and discomfort that the patient may have been previously experiencing.
*A previous incorrect version of this column was posted by the editor.
Catch previous Facial Aesthetics 101 columns
- The growing trend of dissolving filler
- Zoom face: how the pandemic caused a massive surge in aesthetics
- The clinical anatomy of aesthetics
- The initial consultation.
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.

