 Stephen Quinn shares the case of a patient requiring implant treatment following traumatic decoronation of the upper right central incisor.
Stephen Quinn shares the case of a patient requiring implant treatment following traumatic decoronation of the upper right central incisor.
This female patient in her mid-40s was referred to the practice following a traumatic event that resulted in decoronation of the UR1 but was otherwise in good health.
Prior to coming to the practice, the referring dentist had discussed the possible treatment options with her. And she had chosen to have a dental implant placed.
Preparing for treatment
Once the clinical and pre-operative assessments were completed, it was clear that she had good keratinised tissue and a medium smile line.
A radiographic assessment using CBCT was completed. This confirmed sufficient apical bone volume for immediate implant placement.
The required guide was designed using Codiagnostix software. This enables the planning of dental implant insertions precisely and easily.
When carrying out immediate implant placement, it is essential to engage the bone palatal and apical to the root. This allows for good primary stability and insertion torque.
Next, good quality alginate impressions were taken. These were sent to Quoris 3D for printing and, in due course, the guide was delivered with a printed PDF of the plan. This was fixed to the wall on the day of surgery to keep the protocol in the clinician’s line of sight.
Care in the chair
Local anaesthetic was delivered using articaine. Once the patient had confirmed the anaesthetic was working, a three-sided flap was raised. Buccal bone grafting was required and visualisation is key.
The root was then carefully removed, ensuring the buccal plate was left intact. The guide was then checked in place to confirm a passive fit.
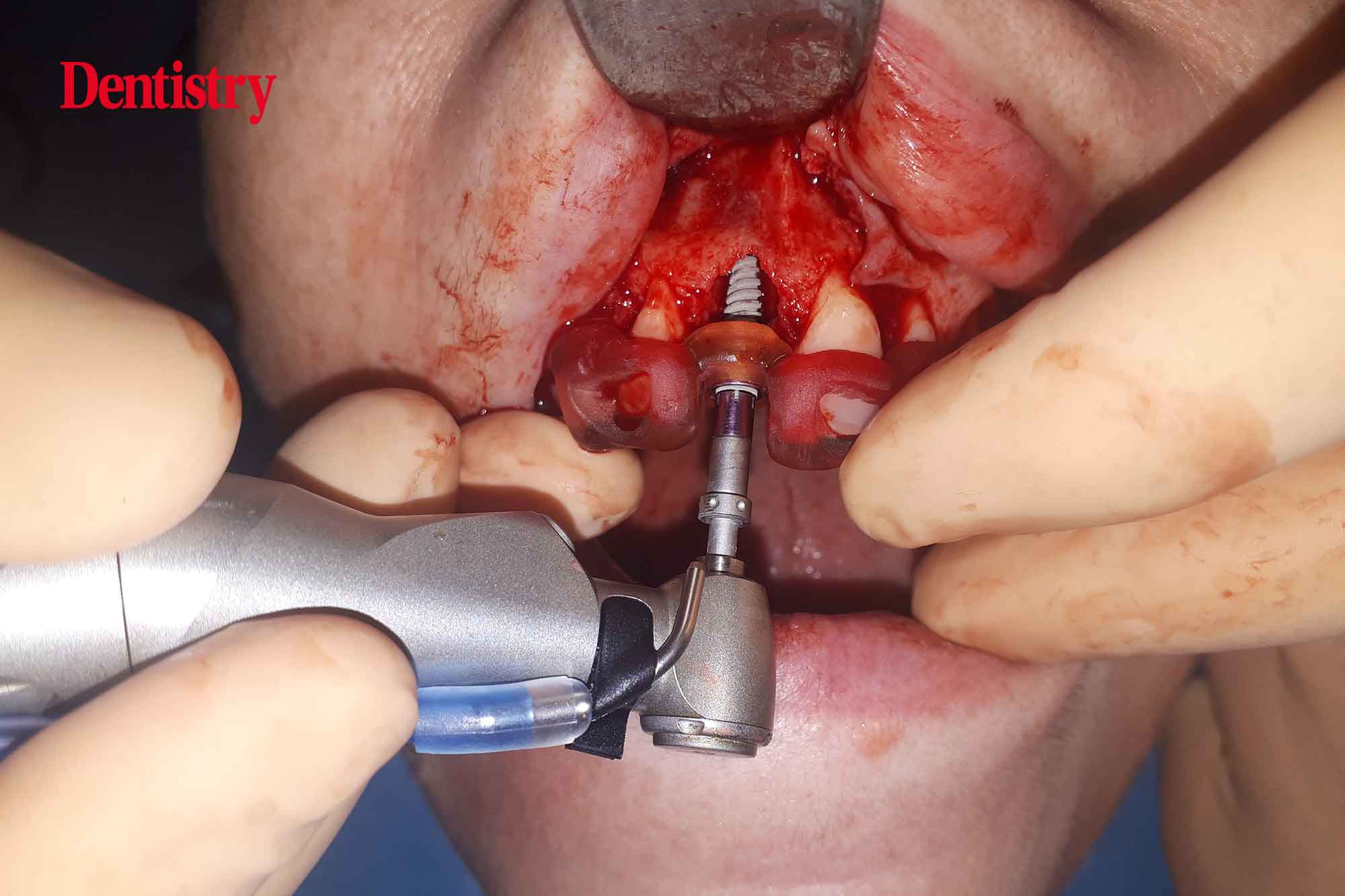
Next, an osteotomy was prepared to the predetermined length, ensuring no lateral movements. The guide had been designed to engage both palatally and apically to the root socket.
Next, the implant was inserted to 45Ncm torque, again confirming good primary stability and insertion torque. This is key had the patient wished to have the tooth immediately restored with a temporary crown.
A periosteal-relieving incision was performed pre-grafting to allow for tension-free closure.
Approaching the end of the appointment, autogenous bone chips were collected and applied to the implant surface. As well as application of a layer of xenograft with a resorbable membrane.
The resorbable membrane was held in place by the healing cap and tension-free closure was performed using resorbable sutures.
Following this successful surgery, at the appropriate time the patient returned to her referring dentist for the restoration to be placed.
 Figure 1: Pre-operative situation with decoronated UR1
Figure 1: Pre-operative situation with decoronated UR1







Chrome, available exclusively through Quoris 3D in the UK and Ireland, offers pioneering full-arch stackable guide technology. It was developed for dentists who desire a pre-planned, predictable guided ‘All-On-X’ type of surgery.
In its entirety, the Chrome service delivers anchored bite verification, anchored bone reduction, anchored site drilling, accurate anchored provisionalisation, and a method of transferring all surgical and restorative information for the final restorative conversion phase.
For further information, please visit quoris3d.com or email [email protected].

