Erosive tooth wear is prevalent in the UK and the number of people presenting with signs of the condition is increasing, Pronamel says.
According to the Adult Dental Health Survey, over three quarters of dentate adults (77%) showed some tooth wear in their anterior teeth, 15% showed moderate wear and 2% showed severe wear (Health and Social Care Information Centre, 2011). Research in Europe highlighted that up to one in three young adults (aged 18-35) exhibit signs of enamel wear (Bartlett et al, 2013).
Tooth wear is a progressive condition that may have lifetime effects, both cosmetic and structural (Harding et al, 2010), highlighting the importance of early intervention and discussion with patients around diet and dietary habits to assess risk.
Is erosive tooth wear recognised and recorded in practice?
A recent study by O’Toole et al (2014) highlighted the fact that tooth wear does not often form part of new patient examinations, particularly amongst established dentists. The BEWE tool was the most common screening tool, however use was predominantly amongst foundation dentists. This may mean that early signs of the condition are not identified.
| Foundation dentists (n=85) | Dentists with 10+ years’ experience (n=200) | |
| % of examinations where tooth wear was charted | 48.2% | 5% |
| % of examinations where tooth wear risk assessment performed | 64.7% | 9.5% |
Causes of erosive tooth wear
Modern diets and lifestyles bring increased challenges to enamel. The move to healthier diets and more frequent snacking throughout the day expose teeth to more frequent acidic challenges.
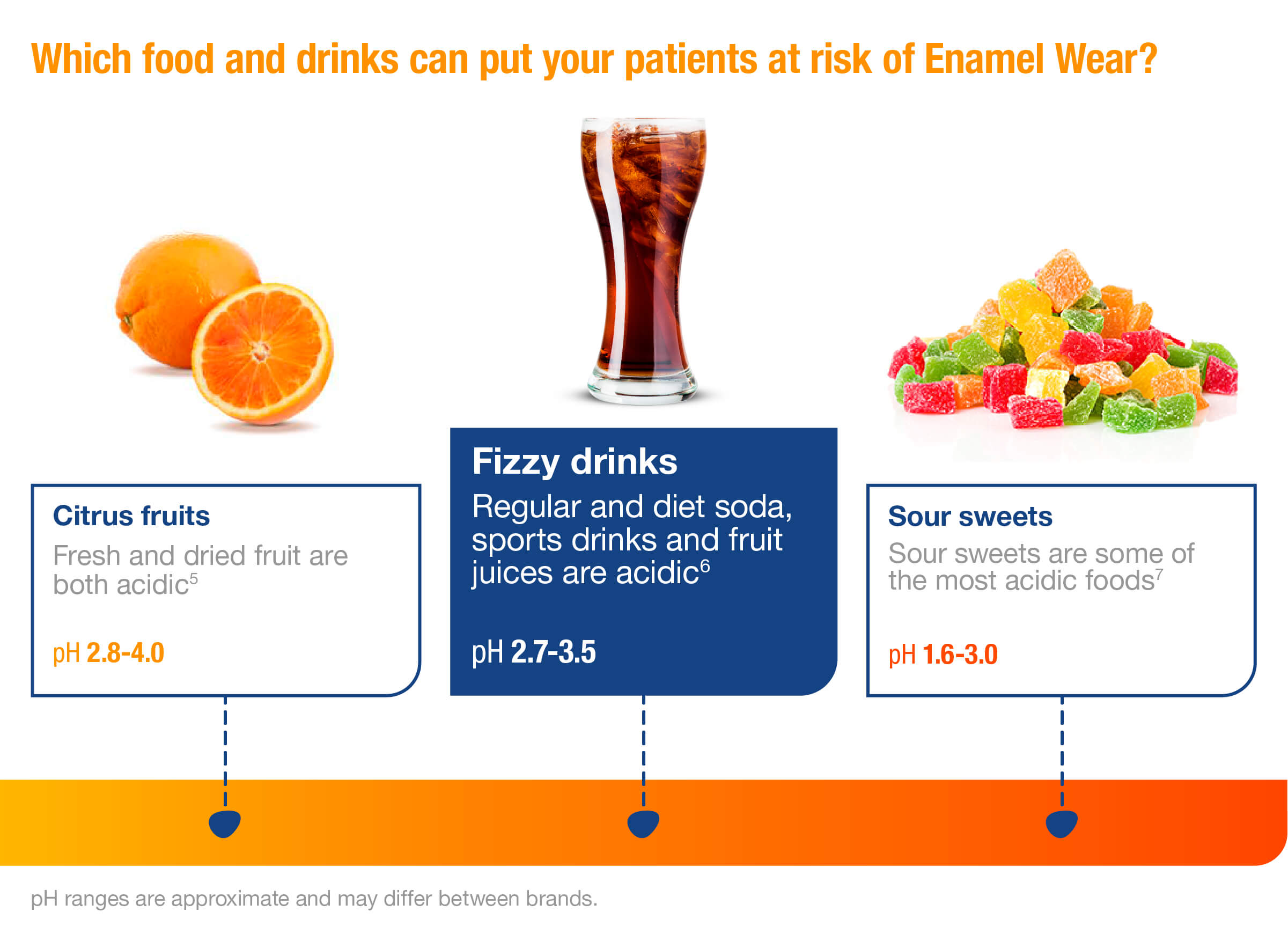
Enamel is equipped to respond to normal daily acid challenges and our mineral rich-saliva ensures that the natural dynamic cycle favours remineralisation. However, frequent or prolonged acid consumption may result in demineralisation and loss of important calcium and phosphate minerals (Mason, 2009).
Once enamel has gone it’s gone for good and so prevention of damage and removal of risk factors are the key to managing erosive tooth wear. In addition, fluoride plays an important role in strengthening enamel and making it more resistant to acid attacks.
Essential patient advice
- Discuss dietary habits with patients and help them to minimise exposure to acids – limit number of challenges a day to less than four (Dugmore and Rock, 2004)
- Brush with an appropriate technique and timing – avoid brushing immediately after consuming acidic food and drinks
- Use a specialised fluoride toothpaste.
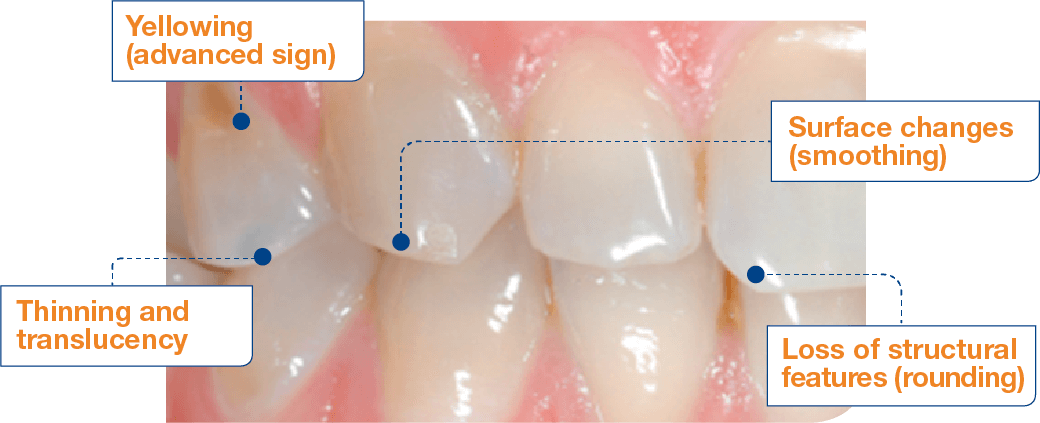
The early signs of enamel wear can be difficult to identify (Lussi, 1996; Lussi, 2006), which means that often initial damage may be left unrecognised. This highlights the importance of monitoring for the condition as well as discussion with patients around diet and dietary habits to assess likelihood of risk.
The role of a specialist toothpaste to help protect against erosive tooth wear
Pronamel has a unique formulation that delivers superior fluoride uptake* for patients at risk of enamel wear (GSK data on file). Pronamel provides dual protection of enamel everyday – by enhancing remineralisation of enamel and inhibiting demineralisation (GSK data on file).
Unlike non-optimised toothpastes, Pronamel is formulated without certain components known to inhibit fluoride uptake by interfering with fluoride binding to enamel (Layer, 2009).
Pronamel has been specifically designed for patients at risk of erosive tooth wear with a gentle formulation to ensure minimal wear on acid-softened enamel (GSK data on file). It is formulated with a carefully controlled level of abrasivity to help maintain the structural integrity of the enamel surface.
Patient conversation about lifestyle diet is an important part of risk assessment for acid wear. Recommend Pronamel to patients, alongside dietary and lifestyle advice, to help strengthen and remineralise enamel.

*compared to non-optimised fluoride toothpastes
References
Bartlett DW, Lussi A, West NX, Bouchard P, Sanz M and Bourgeois D (2013) Prevalence of tooth wear on buccal and lingual surfaces and possible risk factors in young European adults. J Dent 41: 1007-13
Dugmore CR and Rock WP (2004) A multifactorial analysis of factors associated with dental erosion. Br Dent J 196: 282-6
Harding MA, Whelton HP, Shirodaria SC, O Mullane DM and Cronin MS (2010) Is tooth wear in the primary dentition predictive of tooth wear in the permanent dentition? Report from a longitudinal study. Community Dent Health 27: 41-5
Health and Social Care Information Centre (2011) Disease and related disorders – a report from the Adult Dental Health Survey 2009
Layer TM (2009) Formulation considerations for developing toothpastes suitable for those at risk from erosive tooth wear. J Clin Dent 20(6): 199-202
Lussi A (1996) Dental erosion clinical diagnosis and case history taking. Eur J Oral Sci 104: 191-8
Lussi A (2006) Erosive tooth wear – a multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci 20: 1-8
Mason SC (2009) New in vitro and in situ evidence for a toothpaste formulated for those at risk of acid wear. J Clin Dent 20: 175-7
O’Toole S, Patel M, Khan S, Patel A, Patel NJ, Bartlett D and Mohavedi S (2018) Tooth Wear Risk Assessment and Care-Planning in General Dental Practice. BDJ 224: 358-62

