
Justin Durham and Alexandra Penn break down the latest approach to early diagnosis and self-management of temporomandibular disorders (TMD) in general dental practice.
‘My jaw, face and ear are aching, but no-one knows why.’
All dental professionals have probably heard something like this. A patient arrives, perhaps after seeing other healthcare professionals elsewhere, describing an aching jaw, face, and/or ear, without a clear answer as to why they’re feeling this way. Their GP might have examined and excluded their ear as a source of the pain, a dental colleague may have excluded dental pathology, and the patient is in pain, frustrated by the lack of progress towards helping them and/or providing answers through a diagnosis that they understand.
These types of presentations are far from rare, and the most common cause, once sinister/serious mimicking pathology (<1% of presenting cases) is excluded, is a temporomandibular disorder (TMD) also colloquially known as TMJ or TMJD.
The current collective term TMD refers to a group of 12 common musculoskeletal conditions affecting the temporomandibular joint (TMJ), its associated structures, and the muscles of mastication.
Patients living with a TMD may report a range of signs and symptoms which may include: pain in the jaw, temples, and ears; joint noises such as clicking, popping, rustling, or crackling; changes in their jaw’s range of movement. These signs and symptoms often fluctuate over time, and a headache may be either associated with or caused by TMD. As a result of the myriad of symptoms patients can experience, patients may have understandably sought help from several professions/specialities.
Recent English clinical guidance, developed by the Royal College of Surgeons of England’s Faculty of Dental Surgery (RCSEng) in collaboration with NHS England’s Getting It Right First Time (GIRFT) programme, underscores the importance of a structured, evidence-based care pathway for painful TMD assessment and management. The emphasis of the care pathway is on early recognition of TMD, and early patient education and self-management.
Why jaw pain feels so mysterious
Jaw and facial pain often confound patients and clinicians alike because of the complex anatomy in the face and the nature of pain referral. This can make pain feel like it’s coming from the ear, temple, teeth, or head, despite originating in a masticatory muscle or within the TMJ/associated structures.
TMD, like many other conditions, is biopsychosocial, meaning biological factors including pain and other physiological mechanisms interact with behavioural, psychological, and environmental influences. This does not mean the pain is ‘all in the patient’s head’. Rather, it demonstrates the biopsychosocial complexity of the conditions we face as dental professionals, from a dentally anxious patient with an acute irreversible pulpitis to someone with a pronounced gag reflex. This biopsychosocial complexity is particularly evident and important in any painful condition affecting the mouth or face.
A structured approach for general dental practice
For the general dental practitioner, a practical starting point is to use a screening tool such as the three question 3Q/TMD recommended by RCS Eng/GIRFT to determine the likelihood that TMD is present. This can be followed by a focused history and clinical examination. Look for:
- Facial pain modified or provoked by palpation of masticatory muscles or TMJ, or by jaw movement or function, that is the same as that the patient is reporting. Known as ‘familiar pain’
- Joint noises such as clicking or crepitus that are symptomatic ie, causing change in range of motion or pain
- Red flags that mandate urgent action, such as significant trismus, unexplained weight loss, neurological deficits or suspected infective processes or giant cell arteritis.
Education and self-management first
As with most things in dentistry our most powerful professional tools are explanation, education and reassurance. This is especially the case in TMD as patients may interpret, ‘no dental problems’ as meaning their pain is not real, when they simply haven’t been given the diagnosis in a way that makes sense to them.
A simple way to explain TMD to a patient
(Adapted from Beecroft et al 2023)
Temporomandibular disorders, or TMD, is a term we use to describe discomfort and problems in the jaw joints and muscles. It’s also sometimes known as ‘TMJ’ online. You might notice aching pain, headaches, stiffness, or sounds when moving your jaw. The good news is that high quality and reliable evidence demonstrates that in most people, these symptoms improve over time with patience and diligence when using simple non-invasive treatments.
SSM allows a holistic approach to TMD underpinned by education from the dental professional (see box above) and aims to help guide the rehabilitation required (see box below) to control the TMD.
A simple way to explain self-management
(Adapted from Beecroft et al 2023)
Managing TMD yourself using a range of structured content and techniques can be very effective. Simple techniques like doing gentle jaw exercises, paying attention to your jaw position, and using relaxation methods can really help decrease the nervous system activation and pain intensity. We now know from research that most people do better when they learn these skills rather than relying only on treatments done to them, but we can build other treatments onto self-management. It’s a bit like strengthening and stretching an injured muscle – with some practice over weeks, the jaw can feel much better. You’re not alone in this – we’ll guide you step-by-step through the JawSpace app to help you feel more in control.
For busy dental professionals, the challenge may not be diagnosis – it’s knowing how to prescribe and deliver SSM in practice. Questions like, ‘Which jaw exercises should this patient do?’, ‘For how long?’, ‘Should they follow a softer diet, and for how long?’ are common. That’s where digital tools like JawSpace come in, guiding patients through evidence-based self-management in a structured, consistent way.
JawSpace: bridging clinical care and daily self-management
A key challenge in managing TMD in general practice is supporting patients between visits, where much of effectiveness of care can rely on understanding and engaging with self-management.
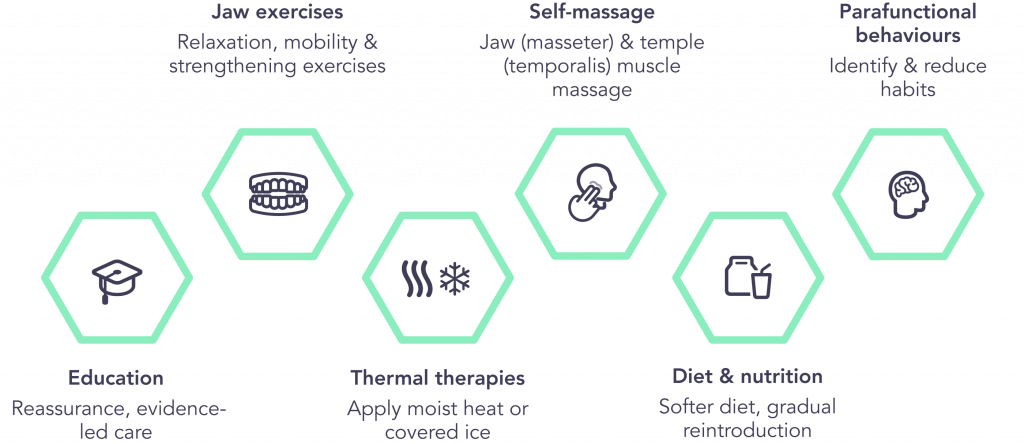
JawSpace is an award-winning digital platform designed to support people with a diagnosed TMD by reinforcing evidence-based self-management between appointments. It offers personalised, evidence-informed guidance across the six recognised pillars of TMD self-management, including jaw exercises, relaxation techniques, habit awareness, and structured symptom tracking.
For dental professionals, JawSpace can help reinforce their in-chair advice, support patient engagement over time, and provide structured symptom reports that can be reviewed at follow-up. The platform integrates easily into practice workflows and includes ongoing continuing education in TMD.
Clinicians can trial JawSpace complimentary for one month and offer it within their practice as a self-management tool for patients.
Why this all matters
Understandably, unexplained jaw, face and ear pain can be extremely distressing for patients. Given the biopsychosocial nature of TMD this can then impact on the condition and cause it to worsen. Structured clinical care pathways, and evidence-based supported self-management early in the course of a TMD is known to be more effective and tools like JawSpace allow that to continue to be reinforced between visits enhancing patient care.
References
- Aggarwal VR, Fu Y, Main CJ, Wu J. The effectiveness of self-management interventions in adults with chronic orofacial pain: A systematic review, meta-analysis and meta-regression. Eur J Pain. 2019 23(5):849-865.
- Beecroft E et al (2023). Management of painful Temporomandibular disorder in adults. NHS England Getting It Right First Time (GIRFT) and Royal College of Surgeons’ Faculty of Dental Surgery. Available from: https://www.rcseng.ac.uk/dental-faculties/fds/publications-guidelines/clinical-guidelines/
- Durham J et al Self-management programmes in temporomandibular disorders: results from an international Delphi process. J Oral Rehabil. 2016 Dec;43(12):929-936.
- Greene CS. Managing the care of patients with temporomandibular disorders: a new guideline for care. J Am Dent Assoc. 2010 Sep;141(9):1086-8.
- Manfredini D et al. Temporomandibular disorders: INfORM/IADR key points for good clinical practice based on standard of care. Cranio. 2025 Jan;43(1):1-5. doi: 10.1080/08869634.2024.2405298. Epub 2024 Oct 3. PMID: 39360749.
- Prodoehl J, Cowley A, Durham J, Lodes M, Rindal B, Mackey S. Bridging the medical-dental divide: a public health imperative for temporomandibular disorders. BMC Glob Public Health. 2025 Nov 4;3(1):97. doi: 10.1186/s44263-025-00217-y. PMID: 41189035; PMCID: PMC12587699.
- Schiffman E, et al . Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache. 2014;28(1):6-27.

