Andrew Chandrapal reveals his non-negotiable products and how they contribute to clinical success.
Dental trauma takes form in various ways but commonly affects the anterior dentition. Some anterior trauma involves concussion to a span of teeth, soft tissue and or the alveolar bone. Other times it can result in subluxation, avulsion or fracture of the alveolus (Lauridsen, 2023).
This case highlights the restorative workflow when the injury involved a single central incisor. The restorative workflow and subsequent prognosis of the restoration is highly dependant on a number of factors:
- Nature of tooth fracture and volume of remaining coronal tissue
- Pulpal tissue involvement both at the time of trauma and in the future
- Disinfection of tooth surface to be bonded to
- Isolation for optimal moisture control during restorative application
- Bonding technique and medicaments
- Occlusal relationships, vertical and horizontal clearance
- Type of restoration, direct/indirect and materials used
- Structured build up of restoration – suitable workflow
- Aesthetic idealism with suitable materials
- Pre operative and posterior operative patient maintenance
- Oral hygiene and plaque control
- Pathological and occlusal changes over time
- Functional and aesthetic expectations of the patient over time
- Frequency of clinical follow-up and recall.
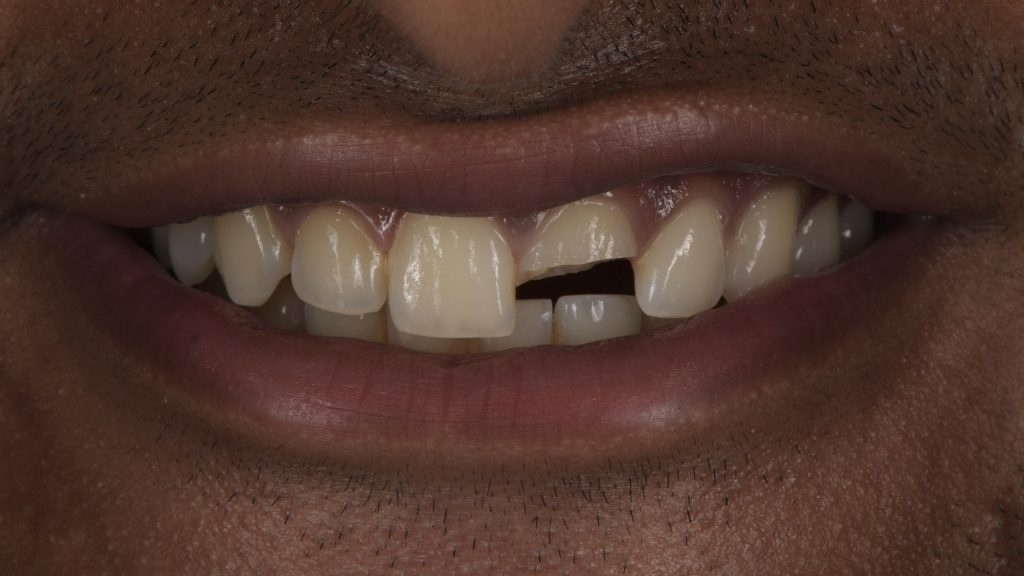
This case was referred to the author as a result of a road traffic accident the patient had been involved in. This had resulted in minor injuries including a substantial fracture to tooth 21. Such was the nature of the fracture, enamel, dentine and pulp tissues were exposed with no recovery of the fractured piece of tooth. As such, the patient’s dental practitioner referred the patient to a specialist endodontist who carried out root treatment thus ensuring the tooth was free from pathology and patient free of symptoms. The patient was then referred for restorative application.
Assessment
First appearance led to a routine restoration of 21 with either direct or indirect materials. Given the age of the patient (21 years old) a decision was taken to attempt a direct restoration that could be converted in the future to an indirect material if and when indicated. This is shown in the extra oral image (Figure 1) where a moderate lip line and average tooth exposure is noted (Chu, 2007).

When further assessment was made tot he intra oral status it was then noted that in maximum intercuspation (MIP) the vertical or inter occlusal clearance between upper and lower incisors was very limited. This can be seen where the mesial palatal aspect of tooth 21 is in direct contact with tooth 31 (Figure 2).
This would place a high load onto any restorative material which could result in premature failure. Identification of such risk factors is key when deciding on how to manage the occlusal relationships that perhaps were not of concern when the dentition was full intact (Kois, 2007).
This also required essential communication to the patient so they understand the need for occlusal management as well as restorative management of the affected tooth. In conclusion to the restorative assessment, it was deemed that the occlusal vertical dimension required opening ion order to create clearance for a direct restorative material to be placed.
The patient was unrestored and so a decision to place direct composite not only to tooth 21 but also to the lower canines, premolars and molars was taken in order to facilitate a stable occlusal pattern that under load could maintain despite being additive composite by having bilateral simultaneous posterior contacts in the absence of immediate contact for the upper anterior incisors with the opposing incisors.
In addition to this, the restorative-natural tooth ratio required greater levels of mechanical retention given the restoration was to be a partial coverage direct composite and not a full coverage indirect restoration and so the coronal aspect of the root canal space was also to be used alongside a suitable direct fibre post.
Operative procedure


The shade and morphological characteristics of the anterior teeth were first recorded using standard light photography in a timely manner to avoid dehydration of the teeth altering the optical properties of the teeth. This can be seen where a black contrastor was used to ensure features such as incisal translucency, halo and intensives were recorded accurately for replication where necessary (Figure 3).
It was also important to communicate such features to the patient when deciding on the aesthetic strategy. This patient was desperate to have a functioning tooth replaced and less concerned about intimate features. However, the author advised on replication of as much as possible. This was accepted by the patient.
Figure 4 shows the teeth under isolation (Heavy Gauge Latex Free Rubber Dam – Unodent, Dental Directory). No claps were used in retention of the isolation but instead rubber ligation and dental tape was used to maintain isolation stability (Wedgets – Coltene, Satin Tape – Oral B). This was all placed using no anaesthesia ensuring comfort for the patient. Note that the floss ligature assists in dental dam inversion into the palatal tissues. At this point the access cavity for root treatment is also visible and so placement of a fibre post was then considered.
It was essential that radiographic assessment of the root treatment was conducted as well as predictable removal of the coronal aspect of the root canal filling material. The tooth was also sandblasted at this point in order to remove any biofilm that would contaminate the bonding process.

Materials used to remove the biofilm (29m aluminium oxide – Velopex International) did not affect both adjacent teeth nor surrounding soft tissues – hence one of the many advantage of optimal isolation. A suitable fibre post (Red 1.25mm Parapost – Coltene) was selected as well as confirmed to fit well and in the correct long axis so as not to interfere with the planned incisal edge and then seated using a resin adhesive (Rely x Unicem – Solventum) being careful to not cover any enamel. Figure 6 illustrates fibre post and angle of placement.


Looking at Figure 6, it also illustrates the resultant position of post placement from the coronal view. It is important that this is placed more towards the palatal aspect so as to not interfere with the layered build up of the direct restoration. The remainder of the tooth was etched (iBond etch – 35, Kulzer) using a selective etch technique. The tooth was then lightly air dried and a universal bonding agent (iBond Universal, Kulzer) was then placed, thinned and light cured.
Given the change to occlusal vertical dimension no mock-up was conducted a freehand thin palatal shell was constructed in a translucent shade of composite resin (CL Venus Pearl – Kulzer).


Composite dentine (OMC Venus Pearl – Kulzer) was used to hold the large palatal shell in place alongside a curved anatomical matrix band (Lumi Contrast – Polydentia) wedged to the intact distal wall of the tooth (Figure 8). Note distal void created but here freehand nature of the palatal shell the would have been avoided had a mock up and stent been used.
Figure 9 highlights the placement of proximal walls (CL Venus Pearl – Kulzer) and dentine mass (OMC Venus Pearl – Kulzer) in to the central aspect of the restorative cavity. Note the post is not not visible. The dentine was arranged into suitable dentine mammelon formation avoiding the incisal edge thus allowing translucency to expose. It was also noted at this stage that the distal wall was over contoured and will require significant reduction during the finishing stage.


The facial application of enamel/effect composite (B1 & CL Venus Pearl – Kulzer) was conducted to complete the mass addition which was placed in such a way to minimise time spent on gross removal (aside from the distal wall). Note the thickness of the separate layers needs to be considered with polychromatic restorations in order to achieve the correct value, chroma and translucency.
Removal of gross excessive volumes from the distal aspect of 21 in order to visualise the final restoration and configure the stages of finishing to include primary, secondary and tertiary anatomy was then required.

Figure 12 shows the immediate post operative extraoral view which is useful to compare shades with the opposing dentition as an indication to rehydrated shade match. The patient also had freehand composite application the to the lower canines, premolars and molars in order to eliminate heavy anterior occlusal loading. It was to ensure these contacts were simultaneous, bilateral and of equal intensity.
The patient was advised they will feel odd for two to three weeks and then feel normal once acclimatisation occurs. A review was arranged for a final finish and polish in seven days.
At the review visit, the patient commented on no issues and was very happy with the outcome (Figure 14). The author notes that ideally more incisal translucency would be ideal. However, the patient remained very happy with the result.


Conclusion
The success of this case remains to be seen for the long term and is currently at a four-year review without issue. Correct occlusal assessment, planning together with rigid application protocols, direct restorative materials with excellent rigidity and aesthetics all make a positive difference to the outcome of such clinical cases.
References:
- Lauridsen E, Andersson L, Suresh N. The Dental Trauma Guide: An evidence‑based treatment guide. Endodontology 2023;35:79-84
- Chu S, A Biometric Approach to Predictable Treatment of Clinical Crown Discrepanices. Pract Proced Aesthet Dent 2007;19(7):401-408
- Kois JC, Hartrick N. Functional Occlusal: Science Driven Management. The Journal of Cosmetic Dentistry 2007, Vol 23:3.
This article is sponsored by Kulzer.

