The Aligner Dental Academy introduces the SAFE assessment system for conducting a comprehensive orthodontic assessment.
Modern dentistry is no longer about simply correcting crooked teeth or closing spaces. It demands a broader and more holistic perspective – one that considers all aspects of the face: facial aesthetics, occlusal function, dental structures and the biology of the soft tissues.
The most predictable and stable results come from ensuring that all these factors are assessed and considered when planning the treatment goals.
The SAFE assessment system, developed by Dr Raman Aulakh, specialist orthodontist, provides a structured and ethical framework for comprehensive dental evaluation. SAFE, representing stability, assessment, function and ethics, integrates orthodontic and restorative principles into a single, cohesive diagnostic pathway applicable to all dental patients.
Designed to ensure consistency and reproducibility across clinicians and treatment modalities, the SAFE system is informed by the principles of facially generated treatment planning.
Assessment begins with the face and smile before progressing to occlusion, tooth structure, and biological considerations, allowing clinicians to prioritise long-term stability and biological safety over appliance-driven decisions.
At its core, the SAFE Assessment System evaluates four key domains: aesthetics, function, structure and biology. This systematic approach supports early risk identification, clear treatment goal formulation, and ethically sound, patient-centred care aligned with the principles of comprehensive dentistry.
Here is a useful document by the Aligner Dental Academy on how to complete the SAFE assessment.
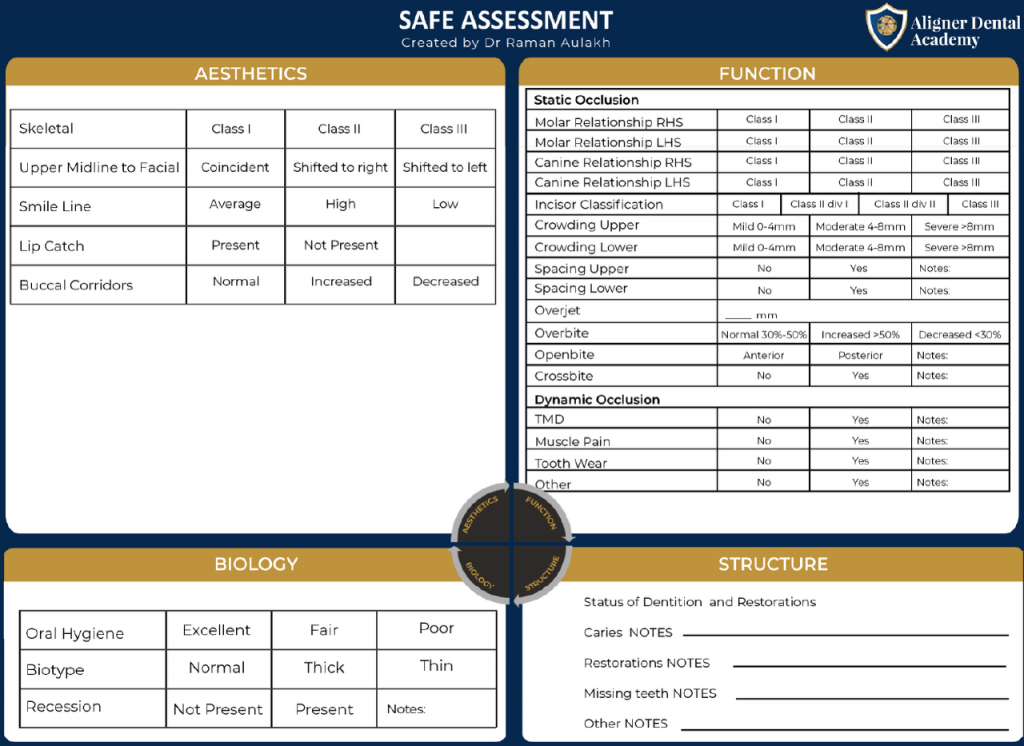
Aesthetic assessment
Aesthetic evaluation begins with the face rather than the teeth. Skeletal relationships are assessed and classified as Class I, II, or III based on the anteroposterior relationship between the maxilla and mandible.
Vertical facial proportions are also examined using anterior lower face height to identify increased, normal, or reduced facial dimensions.
These skeletal findings influence smile balance, lip support, and the feasibility of orthodontic camouflage.
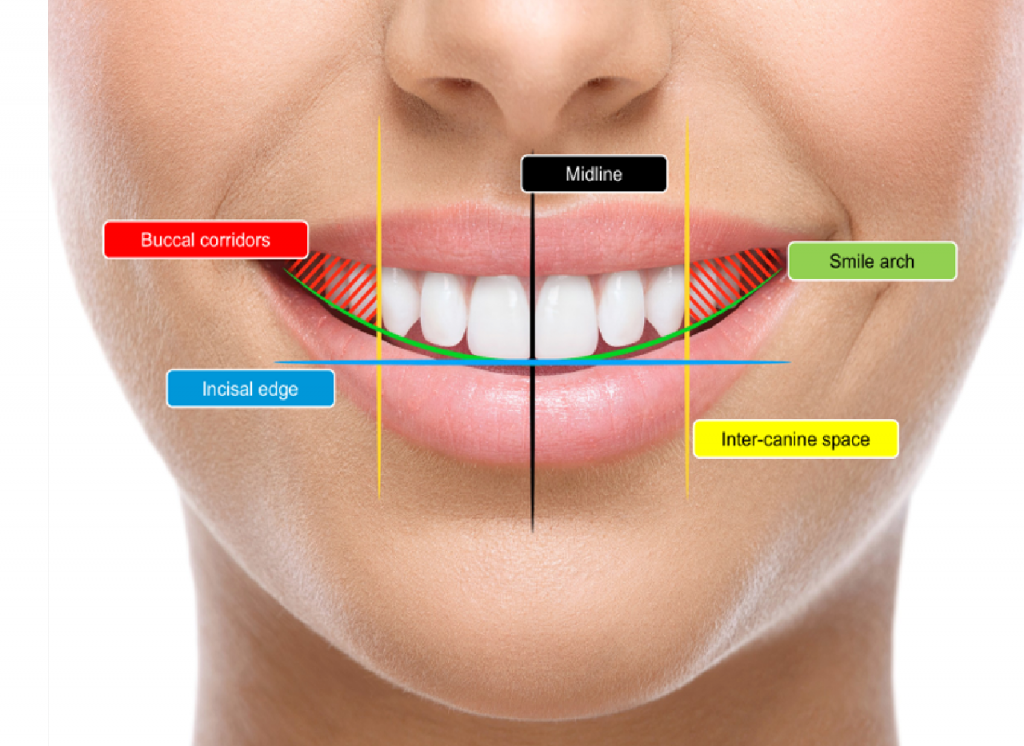
Further aesthetic assessment includes the relationship between the upper dental midline and the facial midline, smile line height, lip dynamics, buccal corridors, and the naso-labial angle.
Features such as lip catch often indicate underlying issues with incisor position or inclination.
This systematic facial and smile analysis allows clinicians to define realistic aesthetic goals that respect individual facial characteristics.
Functional assessment
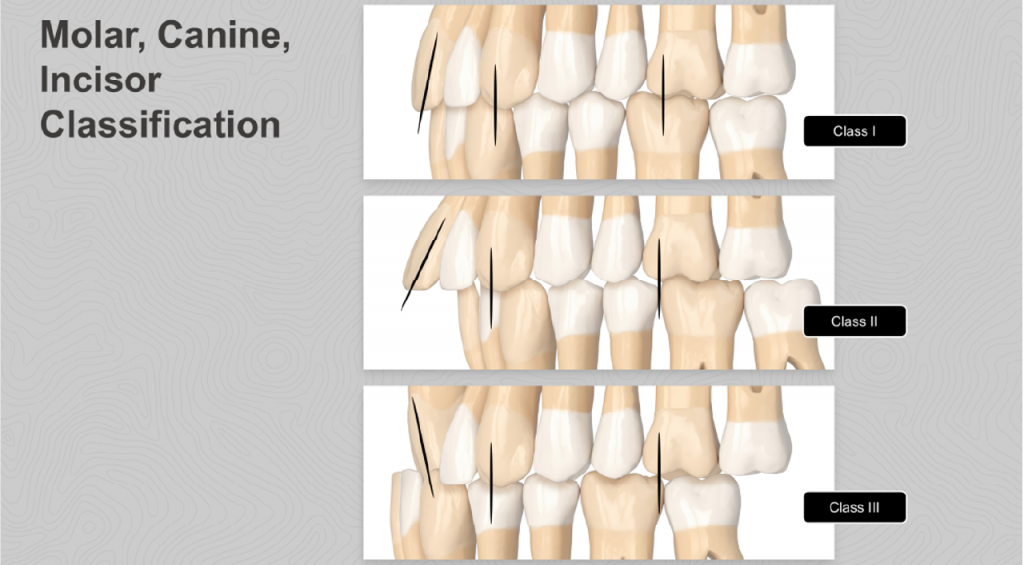
Functional analysis within SAFE is divided into static and dynamic occlusion.
Static occlusion is evaluated with the teeth in maximum intercuspation, documenting molar, canine, and incisor classifications, as well as crowding, spacing, overjet, overbite, open bites, and crossbites. These findings provide a clear picture of the patient’s occlusal relationships and guide orthodontic mechanics.
Dynamic occlusion assessment extends beyond tooth contacts to include temporomandibular joint symptoms, muscle pain, tooth wear, and functional interferences. This ensures that proposed treatments do not worsen existing dysfunction or create new occlusal instability. By integrating static and dynamic findings, SAFE supports functional harmony rather than purely cosmetic correction.
Structural assessment
Structural assessment focuses on the condition of the dentition and existing restorations.
Caries, restorations, root canal treatments, crowns, veneers, missing teeth, and implants are all recorded.
Tooth wear and size discrepancies are also evaluated.
Understanding these factors is essential when planning tooth movement, space closure, or restorative enhancement, as compromised tooth structure can limit treatment options and affect long-term prognosis.

Biological assessment
The biological component of SAFE evaluates periodontal and soft tissue health.
Oral hygiene is graded as excellent, fair, or poor, influencing treatment timing and risk management.
Gingival biotype is assessed and classified as thin, normal, or thick, as thin biotypes carry a higher risk of recession during orthodontic movement.
Existing gingival recession is documented and measured, with SAFE explicitly discouraging labial root movement in areas with reduced periodontal support. This reinforces the ethical foundation of the system.
From assessment to ethical treatment planning
Following assessment, observations are converted into clear treatment goals on whether to accept, improve or correct the condition.
Multiple treatment options can then formulated and discussed with the patient, promoting shared decision-making and informed consent.
Importantly, SAFE emphasises the ethical responsibility to treat or refer, acknowledging that some cases are better managed by specialists or through alternative approaches.
The SAFE system also introduces a concise four-sentence treatment prescription, summarising the patient’s main concern, upper anterior aesthetic goals, space or expansion strategy, and desired overjet and overbite. This improves communication within interdisciplinary teams and enhances treatment predictability.
Conclusion
The SAFE assessment system provides a comprehensive, ethical, and repeatable framework for modern dental practice. By integrating aesthetics, function, structure and biology, SAFE enables clinicians to deliver stable, biologically sound and patient-centred outcomes. In an era of accelerated and simplified dental treatments, SAFE serves as an essential safeguard for quality, ethics, and long-term success.
This article is sponsored by the Aligner Dental Academy.

