 In the first of a new series Exploring Endodontics, Jonathan Murgraff looks at difficulties with silver point endodontic fillings.
In the first of a new series Exploring Endodontics, Jonathan Murgraff looks at difficulties with silver point endodontic fillings.
During the previous century in the 1930s and till several decades later, silver point endodontic fillings were common place (Dubrow, 1976; Bellizzi and Cruse, 1980; Jasper, 1933). And there are still numerous amounts of teeth in the population containing these silver points that will need a retreatment rather than apical micro-surgery or extraction.
Each individual case is always assessed on its own merits. Clearly, silver points have some merits after its use for so long. These are for the following reasons:
- The silver is bactericidal in nature (Gosheger et al, 2004; Percival, Bowler and Russell, 2005)
- The silver endodontic point is very clear on the radiograph. The terminus is very clear on the radiograph due to its radio-opacity compared to gutta percha (Hansrani, 2015)
- The silver points are quite stiff and easy to handle. They are easy to place into position without bending or crimpling of the material (Gerstein, 1983).
Silver point problems
The silver point has enjoyed clinical and radiographic success rates to a certain degree. However, modern endodontic systems and materials produce better and more predictable results than the old silver point filling (Natkin, Van Hassel and Steiner, 1969).
The reason for the progression away from this filling is a result of the following disadvantages associated with silver point:
- Silver points cannot be condensed or compacted on their own to achieve a three-dimensional obturation that alone would allow microleakage (Vishwanath and Rao, 2019)
- The silver point relies on sealer/cement or gutta percha placement around itself to create an apical and complete seal (West, 1987)
- Corrosion of the silver point could result in apical inflammation or argyrosis (Goldberg, 1981; Brady and del Rio, 1975)
- The corrosion of the silver point could result in staining of the tooth
- Presence of the silver point can hinder the creation and placement of a post if needed to restore the tooth
- Root end surgery and retrograde filling is hindered by the presence of a silver point
- The silver points are easily damaged or softened by ultrasonics. And the point can separate and is therefore very difficult to remove.
If 4-5mm of the silverpoint is not left above the canal orifice, the retrieval of the silverpoint in a retreat case is much harder.
Retrieval of the silver point
We can achieve retrieval of the silver point by Stieglitz forceps grabbing the silver point if enough of it is standing proud of the canal orifice. If this cannot be achieved, placing Hedstrom files alongside the silver point, then twisting the files, thus gripping the point, results in the retrieval when the files are withdrawn from the canal. This is a technique as known as brading (Lohar et al, 2019).
Another technique is placing a hollow tube or an applicator tip wide to fit over the tip of silver point. The tube is filled with cyano-acrylate or composite and placed over the silver point.
When the composite sets, the applicator is essentially glued to the tip of the silver point. This is then pulled out (Spriggs, Gettleman and Messer, 1990).
Below are two clinical cases where the teeth are retreated when silver points were in place.
Case one
This patient was referred for retreatment of the LL6 molar tooth that had been previously root treated and restored with a crown more than 30 years ago.
The patient was complaining of pain on biting. Clinical presentation revealed recession of the gingival tissue, but there was minimal pocketing.
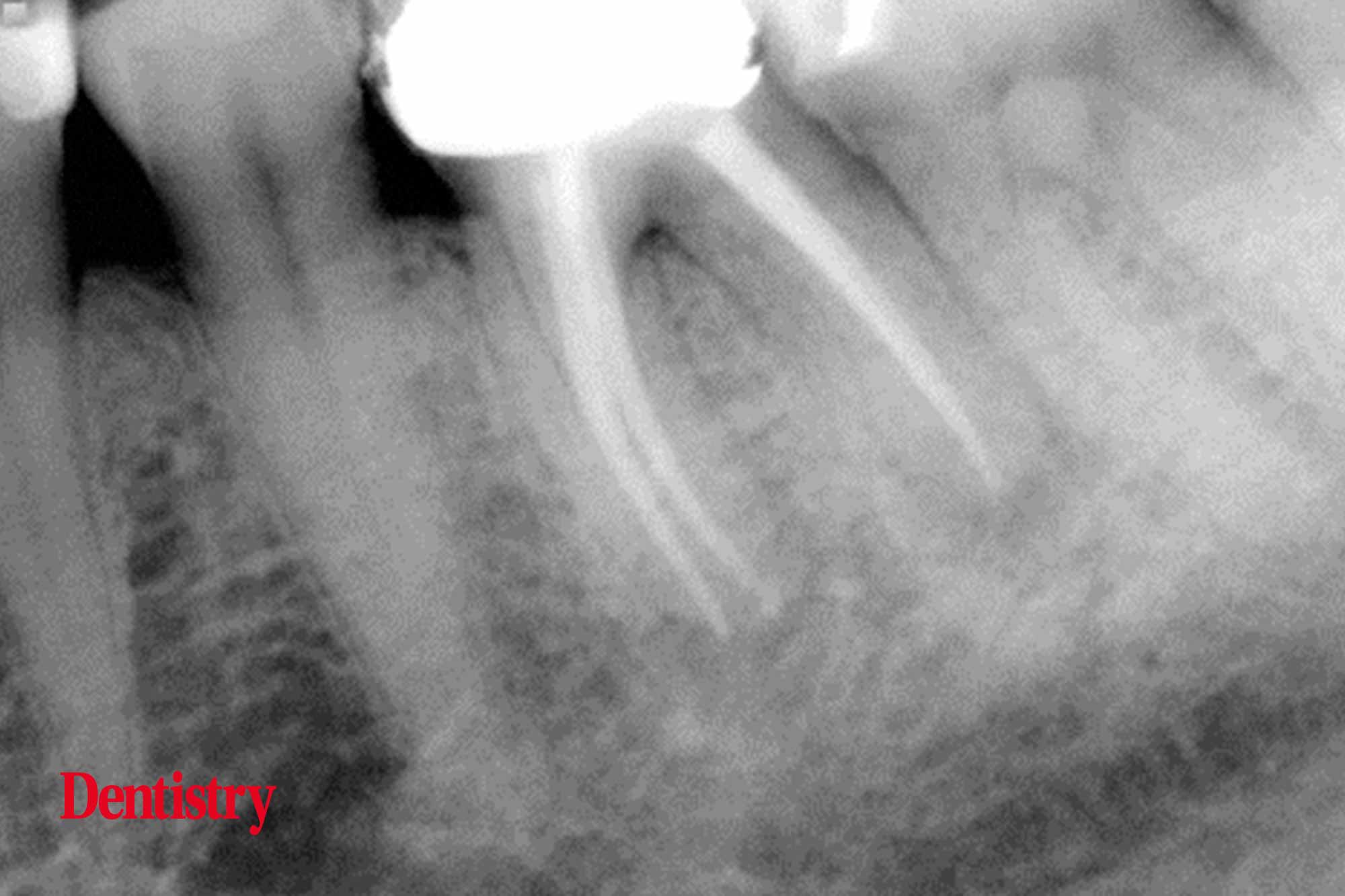
Radiographic presentation revealed an apical area on both roots and with furcation bone loss. But this was commensurate with the general crestal bone level and not suggestive of fracture in the pulpal floor area or vertical root fracture (Figure 1).
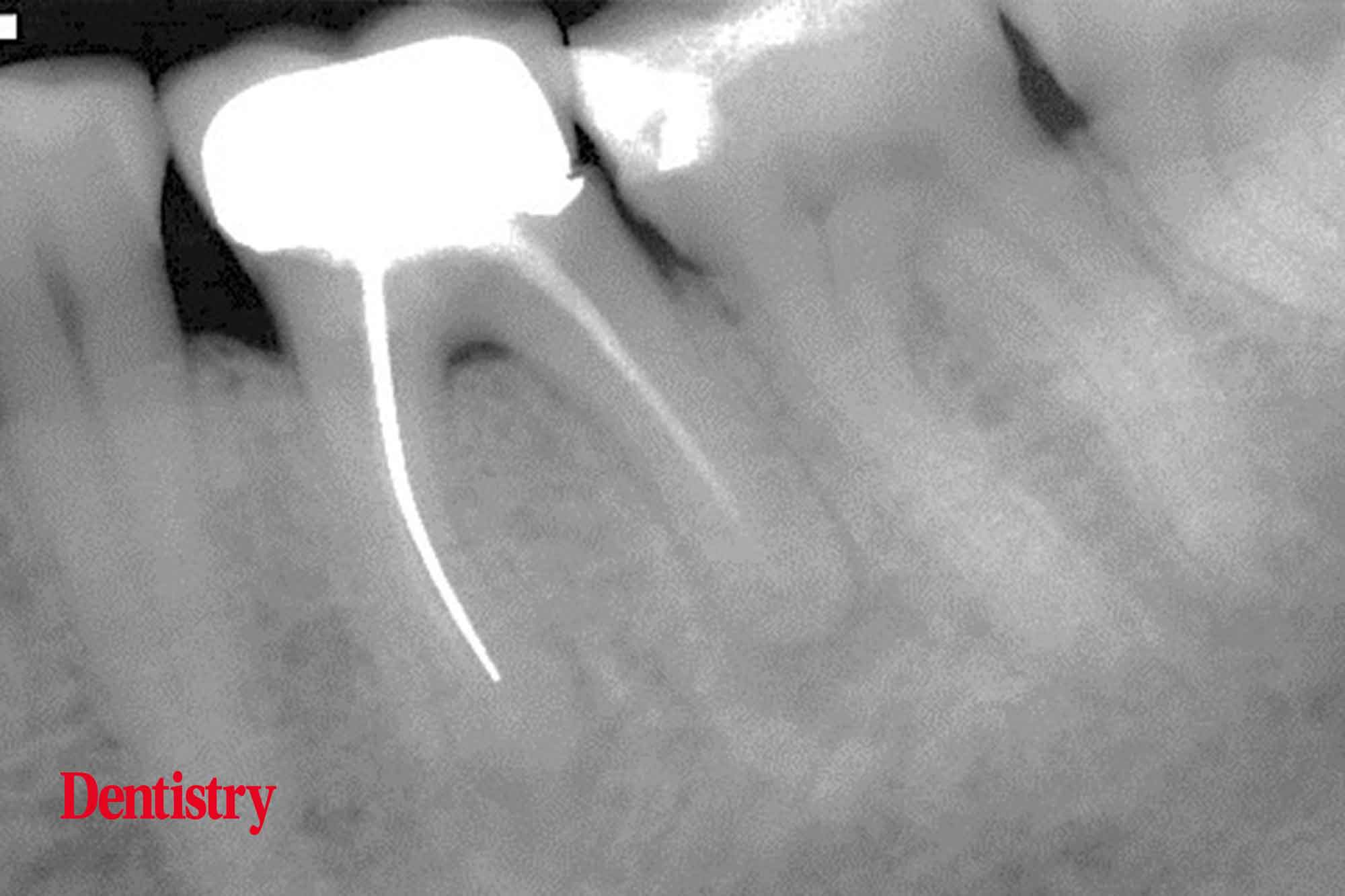
There was no mobility of the tooth and the patient decided to go ahead with re-treatment of the tooth.
It was decided to keep the crown and make an access through this bonded porcelain bonded restoration. The access cavity was carefully made.
Ultrasonic removal of the core was carried out with great care not to touch the silver points with the ultrasonic tip. The coronal section of the silver point was exposed and identified with an operating surgical microscope.
It was possible to attach Stieglitz forceps to the coronal aspect of the point, which was then retrieved (Figure 2).
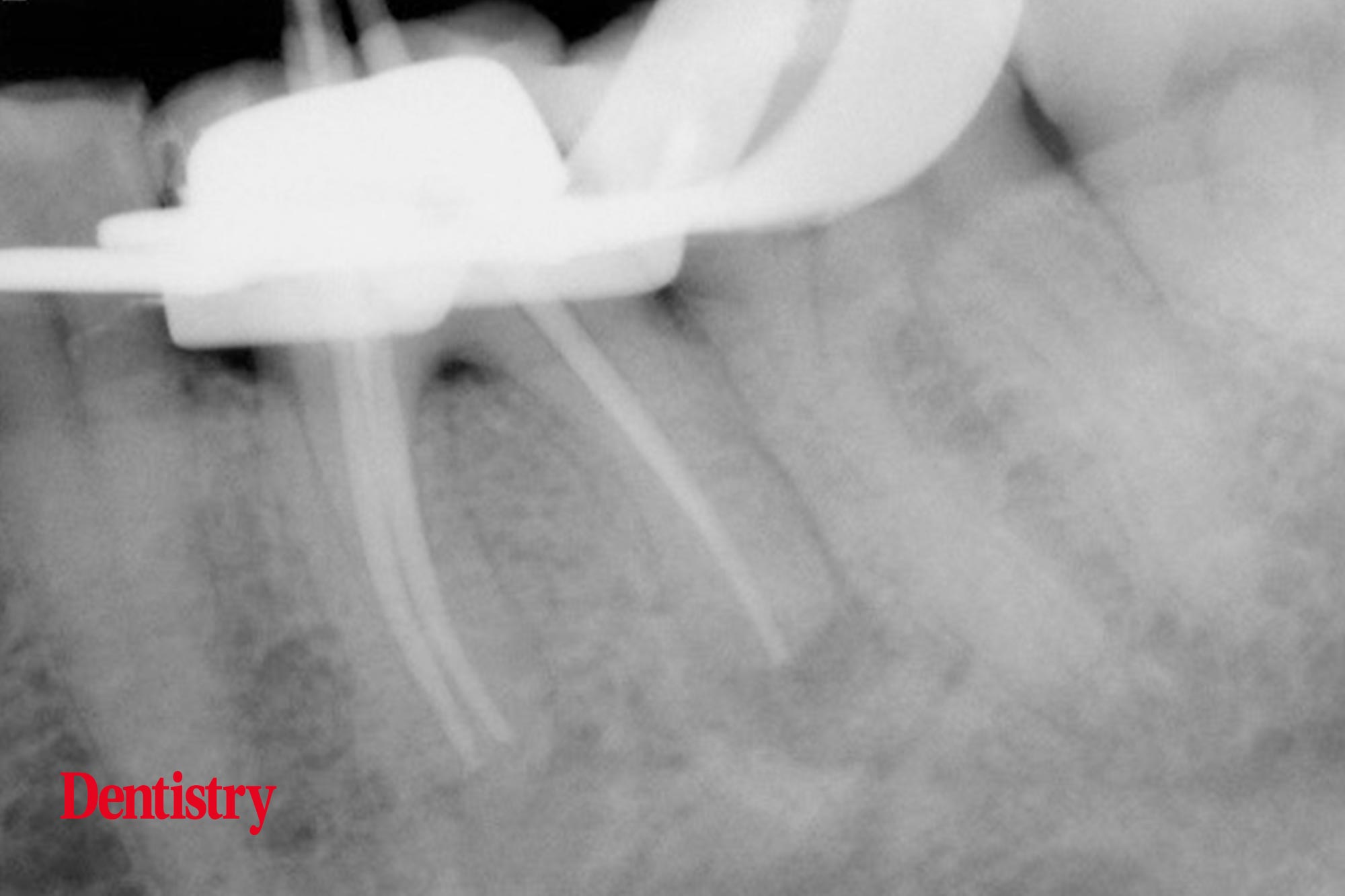
The distal and mesial lingual canal had been operated with Gutta Percha. The removal was carried out using Protaper retreatment file.
We took apex locator readings to assess the working length of each canal. And the final preparation was finished with Protaper gold universal rotary instruments and a working length cone fit radiograph was taken (Figure 3).
We then obturated the tooth using a warm vertical compaction technique. And finally we took a post operative radiograph (Figure 4).
Case two
This was a referred case of a LR6 tooth restored again with a porcelain-bonded crown and had endodontic treatment several decades ago.
The root canal filling was incomplete and the X-ray presentation (Figure 5) revealed apical radiolucencies on both mesial and distal apices.
The apical unprepared portions were in fact very sclerosis and the canals were not seen on the preoperative radiograph.

We preserved the crown and made an access cavity through the crown.
Unfortunately, there was minimal coronal silver point above the canal orifice. Attachment of the point with a Stieglitz forceps was impossible.
We removed the cement around the silver points delicately using the operating microscope throughout. It was then possible to retrieve the silver points by using the brading technique using Hedstrom around the points, which then came out of the canal when removing the Hedstrom files (Figure 6).

We negotiated the apical proportions with a fine flexo-file size 06-10. And the preparation finished with a Waveone reciprocal file.
I obturated the canals with a continuous wave of condensation technique. The parallax radiographic image (Figure 7) shows a slightly widened image of the obturated canals

References
Bellizzi R and Cruse WP (1980) A historic review of endodontics, 1689-1963, part 3. J Endod 6(5): 576-80
Brady JM and del Rio CE (1975) Corrosion of endodontic silver cones in humans: a scanning electron microscope and study. J Endod 205-10
Dubrow H (1976) Silver points and gutta-percha and the role of root canal fillings. J Am Dent Assoc 93(5): 976-80
Gerstein H (1983) In: Techniques in clinical endodontics Philadelphia: L WB Saunders p.259-95
Goldberg F (1981) Relation between corroded silver points and endodontic failures. J Endod 7(5): 224-7
Gosheger G, Hardes J, Ahrens H, Streitburger A, Buerger H, Erren M, Gunsel A, Kemper FH, Winkelmann W and Von Eiff C (2004) Silver-coated megaendoprostheses in a rabbit model–an analysis of the infection rate and toxicological side effects. Biomaterials 25(24): 5547-56
Hansrani V (2015) Assessing root canal fillings on a radiograph-an overview. Br Dent J 219(10): 481-3
Jasper EA (1933) Root canal therapy in modern dentistry. Dental Cosmos 75: 823-9
Lohar J, Sood H, Gosai P and Shekh TM (2019) 3P’s in Retreatment Endodontics-An Often Forgotten Virtue. J Pharm Bioallied Sci 11(Suppl 1): S76-S80
Natkin E, Van Hassel HJ and Steiner JC (1969) The comparative merits of silver cones and gutta percha in the treatment of fine canals of molar teeth. J Br Endod Soc 3(4): 59-61
Percival SL, Bowler PG and Russell D (2005) Bacterial resistance to silver in wound care. J Hosp Infect 60(1): 1-7
Spriggs K, Gettleman B and Messer HH (1990) Evaluation of a new method for silver point removal. J Endod 16(7): 335-8
Vishwanath V and Rao HM (2019) Gutta-percha in endodontics – A comprehensive review of material science. J Conserv Dent 22(3): 216-22
West JD (1987) Endodontic failures marked by lack of threedimensional seal. Endod Rep Fall/Winter: 9

